Gonioscopy is an eye test that uses a special mirrored lens placed on the eye’s surface to directly view the drainage angle. The drainage angle is the structure that determines whether glaucoma is open-angle or angle-closure. Dr Shibal Bhartiya performs gonioscopy in Gurgaon with the room lights dimmed rather than under bright slit-lamp illumination. This is because bright light constricts the pupil and can make a narrow angle falsely appear open.
Gonioscopy is the gold-standard test for classifying glaucoma. The test determines which kind of glaucoma you have. That decision determines whether your treatment is drops, laser, or urgent intervention. Which is why it is extremely important.
If you’ve been told you need a gonioscopy in Gurgaon, it’s worth knowing that not all gonioscopy is done the same way, and the difference affects whether a narrow or closing angle gets caught at all.
Your eye is numbed with anaesthetic drops, so the test itself doesn’t hurt. You may feel mild pressure but not pain. A small amount of gel is placed on a contact lens. the lens is then gently rested on the surface of your eye. You’ll be asked to look in a few different directions while I view your drainage angle through the microscope. The whole test takes about five minutes. Your vision may stay slightly blurry for 15–20 minutes afterward as the gel clears.
What the results mean for you:
Open angle: Your drainage channel is unobstructed. If you have glaucoma, it’s open-angle glaucoma — typically managed with drops, laser, or surgery aimed at lowering pressure over time.
Narrow or occludable angle: Your drainage channel is at risk of closing, even if it hasn’t yet. This changes the conversation from “treat glaucoma” to “prevent an acute attack” — often with a same-visit or near-term laser iridotomy.
Closed angle: The drainage channel is blocked. This is urgent. Untreated angle closure can cause a sudden, painful pressure spike and permanent vision loss within hours to days.
Other findings — pigment deposits, scarring (synechiae), or abnormal blood vessels. These can point to pigment dispersion syndrome, past trauma, or diabetic eye changes. Each redirects your treatment plan differently.
In short: Gonioscopy doesn’t just confirm glaucoma. It decides which kind you have, and that decision determines whether your treatment is drops, laser, or urgent intervention.
Why is Gonioscopy Important?
Gonioscopy is an eye test that visualises the drainage angle of the eye. This drainage angle is responsible for maintaining the eye pressure. Gonioscopy determines if the glaucoma is open angle, or angle closure. It’s findings depend heavily on room lighting and examiner technique. A gonioscopy done under bright slit-lamp illumination can make a narrow angle look falsely open. This is because light constricts the pupil and pulls the iris away from the drainage angle. In Gurgaon, I perform gonioscopy in a dimmed room specifically to avoid this artifact. This way, the angle is graded at its true, physiologic width, not an artificially widened one.
Why Room Lighting Changes the Result
This is one of the most under-discussed variables in glaucoma diagnosis.
When light hits the eye, the pupil constricts. A smaller pupil pulls the peripheral iris away from the trabecular meshwork, which can open up an angle that is, in normal daily conditions, narrow or intermittently closing. If your gonioscopy is done in a bright room, an angle-closure risk can be missed — graded as open when it isn’t reliably open at all.
I do gonioscopy with the room lights dimmed, so the pupil stays closer to its natural size. This is closer to how your eye actually behaves when you walk out of a bright clinic into dim evening light, or sit in a dark cinema. These are the exact conditions in which angle closure is most likely to be triggered. Where indicated, I also use dynamic (indentation) gonioscopy. This involves gently pressing the lens to distinguish a truly closed angle from one that only appears closed (appositional closure). This distinction changes management directly. It decides whether you need a laser iridotomy, monitoring, or nothing at all.
Why Experience in This Specific Test Matters
Gonioscopy is a skill-dependent test — the same eye can be graded differently by two examiners. It takes practiced technique to hold the lens steady, avoid corneal compression that distorts the view, and read subtle angle structures consistently.
Gonioscopy is a routine part of my daily glaucoma practice, not an occasional add-on test. As a fellowship-trained glaucoma and neuro-ophthalmology specialist with over 25 years in the field, and as a research collaborator with Mayo Clinic, Jacksonville, my clinical work is built around glaucoma diagnosis and long-term angle monitoring. This means I perform gonioscopy, not delegate, on nearly every glaucoma or glaucoma-suspect patient I see.
Published Research on Angle Closure
My angle-closure glaucoma work has been published in peer-reviewed journals and is indexed on PubMed, including:
Ultrasound Biomicroscopic Assessment of Angle Parameters in Patients with Primary Angle Closure Glaucoma Undergoing Phacoemulsification — European Journal of Ophthalmology, 2011
Does room lighting really change my gonioscopy result?
Yes. Bright light constricts the pupil and can pull the iris away from the drainage angle, making a narrow angle look artificially open. Gonioscopy done in dim lighting reflects your angle’s true, physiologic width.
What is dynamic (indentation) gonioscopy, and do I need it?
It’s a technique where gentle pressure is applied through the lens to see whether a closed-looking angle is truly closed or only appositionally closed. It’s used selectively, when the initial view suggests possible closure. This is because it changes whether you need a laser iridotomy or just monitoring.
Is gonioscopy available in Gurgaon?
Yes. I perform gonioscopy routinely in Gurgaon as part of every comprehensive glaucoma evaluation. I specifically do it in a dark room, and do the dynamic indentation where indicated.
How is this different from gonioscopy done elsewhere?
The test itself is standardised, but technique varies. Room lighting, indentation technique, and examiner experience all affect the reading. These are the specific variables I control for in every gonioscopy I perform.
Book a Gonioscopy or Glaucoma Evaluation in Gurgaon
If you have a shallow anterior chamber, a family history of angle closure, or have simply never had your drainage angle formally assessed. A gonioscopy — done correctly — is a five-minute test that can prevent an acute angle-closure attack.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Every consultation ends with practical education on how to use eye drops correctly and simple strategies to improve treatment adherence. Successful glaucoma care depends on both accurate diagnosis and consistent treatment.
What Happens During a Glaucoma Consultation? A Doctor’s Walkthrough
Most patients walk into a glaucoma consult expecting a quick pressure check and a prescription. What they get instead, in my clinic, is a sequence. History, vision, anterior segment, a deliberate order of imaging and gonioscopy, baseline pressure testing across more than one visit. The final ten minutes that I consider non negotiable, teaching you how to actually use your drops.
I have refined this sequence over years of glaucoma practice because the disease itself demands it. You cannot feel your eye pressure changing. You cannot feel your nerve fibre layer thinning. The only way to catch glaucoma early and keep it from progressing is a structured, repeatable, slightly unglamorous process. Repeated the same way every single time.
This page walks through that process exactly as it happens in my clinic. So that you know what to expect. It also helps you plan your day better.
Quick Answer: A glaucoma consultation in my clinic moves through five stages. First, the optometrist takes a detailed history and checks vision. This includes uncorrected vision, best corrected vision, and vision with your current glasses. Second, I review that history myself and examine the front of your eye. Third, I run structural and functional tests in a specific order. Corneal thickness, then pressure measurement, then gonioscopy, with OCT and visual field testing done before gonioscopy when they are needed. Fourth, if your pupils need to be dilated, you wait about forty five minutes. Fifth, no consult ends without me personally teaching you how to instil your eye drops correctly and how to remember whether you have taken them.
A look inside a real glaucoma consultation with Dr Shibal Bhartiya in Gurgaon: structured testing order, baseline pressure checks across visits, and personalised target pressure zones that guide treatment decisions before any drop is prescribed.
How to Prepare for Your Glaucoma Consultation
A little preparation before your appointment can make your glaucoma consultation more useful and help your ophthalmologist understand your eyes over time.
If possible, bring any previous eye records, including OCT scans, visual field reports, optic nerve photographs, eye pressure readings, and details of any eye surgery or laser treatment. If you use glaucoma eye drops, bring a list of your medications or the bottles themselves. It is also helpful to know whether anyone in your family has glaucoma or significant vision loss.
Write down any questions or changes you have noticed since your last visit, even if they seem minor. Most importantly, do not stop using your prescribed eye drops before your appointment unless your ophthalmologist has specifically advised you to do so.
The more complete your previous records, the easier it is to compare changes over time—because in glaucoma, understanding what has changed is often more important than any single test result.
Step 1: Before You See Me, the Optometrist Does the Groundwork
Every consult starts with my optometrist, not with me. This is deliberate. It means your history is captured properly and your vision is measured in a structured way before I ever walk into the room.
History taking
The optometrist takes a detailed history and reviews any prior reports, scans, or visual fields you bring with you, noting all of it into your file. This includes systemic conditions that have nothing to do with the eye on the surface, diabetes, high blood pressure, heart disease, asthma, or autoimmune disease, along with any current medications and known allergies. Glaucoma management decisions are frequently shaped by what is happening in the rest of your body, so none of this is skipped.
Three vision measurements, not one
Your vision is then checked through a formal refraction, and three separate numbers are recorded:
UCVA, your uncorrected visual acuity, what you see with no glasses at all
PGP, your vision with the glasses you are currently wearing and prescribed
BCVA, your best corrected visual acuity, what you could see with the ideal glasses prescription
Comparing these three numbers tells me whether a vision problem is about your eyewear, your ocular surface, or your optic nerve, before I have even examined you. A non contact tonometry pressure check is occasionally done at this stage as a screening step. I insist on Goldmann Applanation Tonometry for all of my glaucoma patients.
Step 2: I Review Your History and Examine the Front of the Eye
When you come in to see me, I read through everything the optometrist has documented at a glance. If anything looks incomplete, inconsistent, or worth a second look, I will ask more specific questions to understand it properly before moving forward.
There is also, always, a few minutes of ordinary conversation. A glaucoma consult is a long term relationship, not a transaction. It starts with treating you like a person before a set of test results. And you will be shocked at the details I remember. Your family, your last vacation, your dog 🙂 sometimes, even your favourite chutney!
I then examine the front of your eye in detail. The conjunctiva and ocular surface, the meibomian glands, the eyelid and bulbar conjunctiva, the anterior chamber, and the lens, looking specifically for cataract, a shallow anterior chamber, or any cells in the anterior chamber (inflammation).
Step 3: A Deliberate Order of Testing, Not a Random Checklist
The sequence in which glaucoma tests are performed matters, and I follow a fixed order rather than doing whichever test is most convenient.
Angle assessment first, with imaging informing the decision
I assess the optic nerve with a 90 dioptre lens. Every glaucoma patient gets a gonioscopy. When you need a repeat gonioscopy is decided after that. I perform it only after the visual field test, the OCT, and fundus photography are done, when those are part of that visit. Imaging the nerve and the visual field before manipulating the angle gives me a cleaner functional and structural baseline to work from.
Central corneal thickness, then pressure, then gonioscopy
Before gonioscopy, I measure central corneal thickness (CCT), the test also called pachymetry. Corneal thickness directly affects how your raw eye pressure reading should be interpreted. But it is always done before your tonometry. Because touching your corneas to measure your IOP before the CCT may alter it slightly. Gonioscopy then follows. This examines your drainage angle under magnification. This determines whether you have an open angle or a narrow angle profile.
Why I do the pressure check myself
Goldmann applanation tonometry (GAT), the test that measures your intraocular pressure, is the one test I do not delegate. In my clinic, I personally perform this for every glaucoma patient before treatment starts. Again at the first follow up, and at every annual review. My optometrists are trained to do it and do perform it in my absence. Doing it myself gives me a direct feel for what is happening in your eye that a number on a chart cannot fully convey.
I also insist on doing my gonioscopy myself, always with the lights switched off, so be prepared for a few minutes in a dark room. I keep talking to you, so its never scary.
How is Applanation Tonometry Done?
For the GAT, one of my team members will put some numbing eyedrops and ask you not to touch your eye. I then put a dye which stains your tears yellow. And then I check your eye pressures under blue light on the slit lamp, with a prism that comes close to the eye.
It takes less than a minute if you don’t blink and keep looking straight ahead, and a few extra seconds if you fidget. It’s painless, and quick, and we finish with a drop of antibiotic in the eye.
Step 4: Dilation, When It Is Needed
If your assessment requires dilating your pupils, you will be told this in advance, because dilation takes about forty five minutes to take full effect and changes how you experience the rest of your day.
We ask you to bring dark glasses, a scarf, or an umbrella, since dilated eyes are far more light sensitive, particularly in Gurugram’s daytime heat
We advise you not to drive yourself home after a dilated examination
Step 5: Establishing a True Baseline, Not a Single Snapshot
Glaucoma decisions should never rest on one reading taken on one day. Two specific habits in my clinic exist to correct for that.
Repeating your first visual field
There is a genuine learning curve to taking a visual field test well. The first attempt is frequently unreliable simply because the patient has not yet learned the rhythm of the test. I routinely discard the first visual field and ask patients to return the next morning. We do not charge for that repeat test. The inaccuracy is a known limitation of the test itself, and is not a reason to bill twice.
Three pressure readings, not one
For a true baseline, I usually take three intraocular pressure readings at different times of day. Rather than relying on a single number, since pressure naturally fluctuates through the day. One of these three readings may be taken by an optometrist, if it’s after my working hours. We usually work from the average of all three.
The water drinking test
A formal diurnal variation test, in which pressure is measured every few hours through the day, is not practical for every patient. We often use the water drinking test as a more practical stand in. This is typically done before starting treatment, again about one to two months after treatment begins. We may repeat it if your eye appears to be progressing despite your pressure meeting its target.
Step 6: Setting Your Personalised Target Pressure
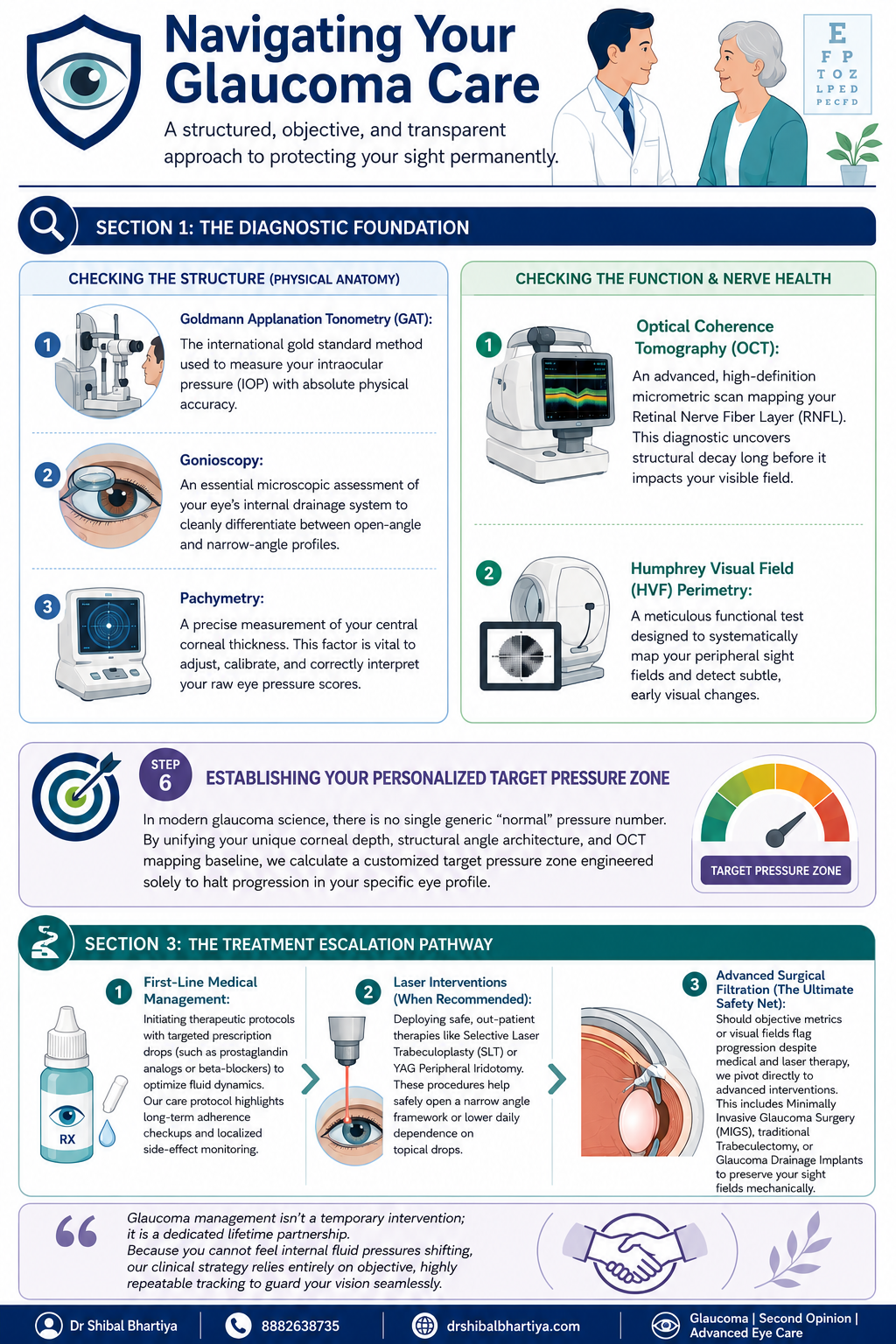
There is no single universal normal pressure number in modern glaucoma care. Your corneal thickness, the structure of your drainage angle, and your Visual field and OCT baseline are combined to calculate a target pressure zone. This is specific to your eye, designed to halt progression for you.
Step 7: The Most Important Section of Glaucoma Consultation: Eye Drop Training
A prescription on its own does not protect your vision if the drops never go in correctly or are forgotten. So every consult ends with practical training, not just instructions.
I personally show you how to instil your eye drops correctly, since technique affects how much medication actually reaches the eye
I ask you to set a phone alarm for every dose. Because relying on memory alone is the most common reason treatment fails
If you are on more than one medication, I recommend keeping two small boxes. One empty and one full of your drop bottles. After each dose, you move that bottle from the full box to the empty one. So a glance at the boxes tells you whether you have already taken that round of drops. And which ones remain.
When you leave, my coordinator helps you set your next appointment, before you leave the clinic. You will also receive a Whatsapp message with links to important information and details of phone numbers to book appointments. You will also get my direct phone number for any clinical queries, or emergencies.
When To See Me Before Your Booked Glaucoma Consultation
Sudden eye pain, redness, or blurred vision, which can signal an acute angle closure attack
Any one sided change in vision or eye appearance
Headache or nausea accompanying eye pain
A noticeable change in your visual field between scheduled visits
New side effects after starting or changing a glaucoma medication
Missed doses for several consecutive days, which should be flagged at your next visit rather than left unmentioned
Why Two Patients With the Same Eye Pressure May Receive Different Advice
It is natural to wonder why one person is advised to start glaucoma treatment immediately, while another with a similar eye pressure is simply monitored.
The answer is that glaucoma is not diagnosed or treated based on a single number.
When I assess a patient, I consider the health of the optic nerve, OCT scans, visual field results, corneal thickness, family history, age, previous eye records, and whether there is any evidence that the disease is progressing. I also take into account your lifestyle, occupation, and life expectancy, because the goal is to preserve the vision you need throughout your lifetime.
Two patients may have the same eye pressure but very different levels of risk. One may benefit from careful observation, while the other may need treatment without delay.
My role is not simply to diagnose glaucoma. It is to understand your individual risk of vision loss and recommend the right treatment at the right time.
Why does the optometrist see me before the doctor does?
The optometrist’s workup, history, refraction, and the three part vision check, ensures your file is complete and your baseline vision is documented accurately before I begin my own examination. This makes the time I spend with you more focused on interpretation and decision making rather than data collection.
Why do you measure my eye pressure yourself instead of leaving it to staff?
Goldmann applanation tonometry is the gold standard pressure test, and for every glaucoma patient I treat, I perform it myself before starting treatment, at the first follow up, and at every annual review. It gives me a direct sense of your eye’s behaviour that I do not want to lose by always delegating it.
Why do you discard my first visual field test and ask me to repeat it?
Most patients have not yet learned the rhythm of the visual field test on their first attempt. This makes that first result unreliable. We ask you to return the next morning for a repeat test. We do not charge for it, since the inaccuracy belongs to the learning curve of the test, not to you.
Why is gonioscopy done after OCT and visual field testing, not before?
When OCT, visual field testing, and fundus photography are part of your visit, I prefer to have that structural and functional picture in hand before manipulating the angle during gonioscopy. The order is chosen to give the cleanest possible baseline. Also, sometimes I use a viscoelastic gel for gonioscopy. In that case, your vision is fuzzy for about ten minutes after, and I don’t want your time wasted.
What is the water drinking test and why would I need one?
It is a practical way of checking how your eye pressure responds to a physiological stress. This is used in place of round the clock diurnal variation testing, which is not feasible for every patient. I typically use it before starting treatment. I may repeat it again a month or two into treatment. And again later if your eye appears to be progressing even though your pressure looks controlled.
Why do you spend time teaching me to put in my own eye drops?
Technique directly affects how much medication reaches your eye. A missed or mistimed dose is the most common reason glaucoma treatment underperforms. Pairing a phone alarm with the two box system is simple. It gives you a simple, visual way to know whether today’s dose has already gone in. Research says it is the most important intervention in preventing glaucoma blindness.
Is Dr Shibal Bhartiya the best glaucoma specialist in Gurgaon?
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist with over 25 years of experience. Her training includes AIIMS New Delhi and the University of Geneva. She is a Mayo Clinic Research Collaborator, has authored over 200 scientific publications, edited 28 ophthalmology textbooks, and has more than 1,600 five-star Google reviews from patients. A lot of her patients call her the best glaucoma specialist in Gurgaon.
What do patients say about Dr Shibal Bhartiya’s care, beyond her credentials?
Patients consistently describe feeling heard, never rushed, and receiving clear, personalised explanations. Many value her ethical approach, thoughtful second opinions, and focus on preserving both vision and quality of life. Many reviews also describe her as the best glaucoma specialist or eye doctor in Gurgaon.
Key Takeaways
Your consult begins with the optometrist. They document history and perform three vision measurements, UCVA, PGP, and BCVA, before I examine you
Testing follows a fixed order: imaging and visual field first when needed, then corneal thickness, then gonioscopy, then pressure measurement
I personally measure your eye pressure for every glaucoma patient at key visits, rather than delegating it
Your first visual field is usually repeated free of charge, because of a genuine learning curve with the test
Baseline pressure is built from three readings at different times of day, sometimes supplemented by a water drinking test
Your target pressure is personalised to your eye’s anatomy, not based on one generic normal number
No consult ends without hands on training in how to use your drops. And how to track whether you have taken them
Book a Consultation
If you have been told you have glaucoma, or are due for a routine check because of family history or elevated pressure, this is the process you can expect to walk through.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
⭐ Helped by this article? Leave a Google review — it helps other patients find reliable eye care.
A Routine Eye Check and Glaucoma
A routine eye check may raise suspicion of glaucoma through elevated eye pressure, changes in the optic nerve, or unexplained vision changes. However, confirming glaucoma usually requires specialised tests such as optic nerve imaging, visual field testing, and corneal thickness measurement. Also, a routine for glasses is not a substitute for an eye exam, as the former can often miss glaucoma.
Glaucoma usually causes no pain, no redness, and no obvious vision change in its early stages. Most people with glaucoma feel completely normal until significant and irreversible damage has occurred. The only way to detect it early is a comprehensive eye examination that includes optic nerve assessment, intraocular pressure measurement, and visual field testing
A Routine Eye Check Revealed a Sight-Threatening Disease
Mrs SG came to see me because her glasses prescription had not felt right for a few months. She was 57. She worked at a desk. Her eyes were tired by evening, and she assumed she needed a stronger number. She had no pain. No redness. No alarming moment that made her think something was wrong.
Her previous optician had given her a new prescription six months earlier. It had not helped. She booked an appointment with me because a colleague had suggested a second opinion.
I examined her in the usual way. Her visual acuity was reasonable. Her anterior segment was quiet. Then I checked her retina and optic nerve.
She did not need a stronger glasses prescription. She had glaucoma, and it had been quietly advancing for what was likely several years.
Patient details have been changed to protect privacy.
Remember
Sunita’s case is not unusual. Glaucoma is called the silent thief of sight for a reason. It causes no pain, no visible redness, and no early warning that most patients would recognise. By the time vision loss is noticeable, the disease has already caused permanent damage. In India, an estimated 12 million people have glaucoma, and almost 90% of them do not know it. (The Chennai glaucoma Study).
Below, I explain what glaucoma actually does to the eye, why it is so reliably missed, and which symptoms, or absences of symptoms, should prompt an urgent examination.
What Glaucoma Actually Does to Your Eye
Glaucoma is a disease of the optic nerve. The optic nerve carries visual information from the eye to the brain. When this nerve is damaged, that information is lost permanently. No treatment can restore what is already gone. Treatment can only slow or stop further damage.
In most cases, the damage is caused or worsened by raised pressure inside the eye. This pressure, called intraocular pressure or IOP, builds when fluid inside the eye does not drain properly. The drainage system becomes less efficient over time, pressure rises, and the optic nerve fibres begin to die. The process is painless in the vast majority of patients.
What makes glaucoma particularly deceptive is the pattern of vision loss. It begins at the periphery, the edges of your visual field. The brain compensates automatically. Both eyes together create a complete picture, and each eye covers for the blind spots of the other. Patients often do not notice peripheral vision loss until more than 40 percent of their optic nerve fibres have already been destroyed. By that point, the disease is well advanced.
In SG’s case, her glasses prescription had changed slightly because her visual system was compensating for early field loss. It was not a refractive change. It was her brain working harder to make sense of incomplete information. This pattern, subtle visual dissatisfaction without a clear cause, is one of the most common presentations I see in patients who turn out to have early to moderate glaucoma.
Glaucoma vs Normal Ageing: How to Tell the Difference
Symptom or Sign
What It Suggests
What To Do
Gradual blurring that a new glasses prescription does not fix
May indicate optic nerve or macular pathology, not refractive change
See an ophthalmologist for optic nerve assessment, not just a refraction
Difficulty adjusting from bright to dim light
Can be an early sign of peripheral field loss
Request a visual field test at your next eye appointment
Frequent glasses changes with no lasting improvement
Suggests the problem is not the prescription
Ask for intraocular pressure measurement and disc evaluation
Mild headache or eye heaviness without redness
In some patients, mildly elevated IOP causes subtle discomfort
Check IOP, especially if over 40 or with family history of glaucoma
No symptoms at all, but a family member has glaucoma
First-degree relatives have a 4 to 9 times higher risk
Schedule a comprehensive glaucoma screening even if you feel completely well
When a patient visits an optician or a basic eye clinic for a new prescription, the standard assessment measures visual acuity and refraction. It does not always include optic nerve photography, intraocular pressure measurement, or visual field testing. These are the three investigations that detect glaucoma. Without all three, the disease is invisible.
Sunita had seen an optician twice in three years. Her visual acuity was checked each time. Her optic nerve was never examined.
The second reason glaucoma is missed is the absence of symptoms. Patients present to doctors when something feels wrong. Glaucoma does not feel wrong, not for years. There is no cultural expectation in India of an annual comprehensive eye examination. Most people attend only when they need a new prescription or when something is visibly red or painful. By those criteria, a glaucoma patient has no reason to come at all.
The third reason is that IOP alone is not a reliable screening tool. Many patients with glaucoma have pressure in the so-called normal range. Normal-tension glaucoma accounts for a substantial proportion of cases, particularly in people of Asian descent. A single IOP reading of 16 mmHg does not exclude the diagnosis.
SG’s IOP was elevated, which made diagnosis more straightforward. But many of my patients with confirmed glaucoma have had pressures that would not have triggered concern at a routine check.
But My Eye Test Was Normal
Many patients tell me, “But I had a routine eye check and everything was normal.” I explain that a routine eye examination and a glaucoma evaluation are not the same thing. My role is not simply to measure your eye pressure. I assess your optic nerve, interpret your OCT and visual field tests, evaluate your risk factors, and decide whether your eyes are likely to remain stable over time.
What does a routine eye check usually include?
Vision testing
Glasses prescription
Eye pressure (sometimes)
External eye examination
Basic retinal examination
What does a glaucoma evaluation include?
Optic nerve assessment
OCT
Visual field
Gonioscopy
Corneal thickness
Risk assessment
When To See an Eye Specialist
See an ophthalmologist for a comprehensive glaucoma assessment if any of the following apply:
A parent, sibling, or child has been diagnosed with glaucoma
You are over 40 and have not had a comprehensive eye examination in the past two years
You have been told your eye pressure is “a little high” but were not referred further
You have changed your glasses prescription twice in two years with no lasting improvement
You have diabetes, as this increases glaucoma risk
You are of South Asian, East Asian, or African descent, all of which carry higher glaucoma risk
You use steroid eye drops, nasal sprays, or inhalers long-term
You were told everything was fine, but your vision still does not feel right
Yes. Normal-tension glaucoma is a recognised and common form of the disease, particularly in people of Asian descent. A normal IOP reading does not rule out glaucoma; optic nerve assessment and visual field testing are essential.
Does glaucoma always cause pain?
No. The most common forms of glaucoma are completely painless. Pain is associated with acute angle-closure glaucoma, which is a sudden and rare presentation. Most patients with chronic open-angle glaucoma, the most prevalent type, feel nothing at all until vision loss is advanced.
Can lost vision from glaucoma be restored?
No. Optic nerve damage caused by glaucoma is permanent. Treatment with eye drops, laser, or surgery can slow or stop further damage, but vision already lost cannot be recovered. Early detection is the only way to protect useful sight.
How often should I have a glaucoma check if I have a family history?
If a first-degree relative has glaucoma, you should have a comprehensive eye examination every year from the age of 40, or earlier if your ophthalmologist advises it.
Book a Consultation
If you have a family history of glaucoma, have not had a comprehensive eye examination in the past two years, or have been told your eye pressure is elevated, a dedicated assessment is worth arranging now. The earlier glaucoma is found, the more vision can be protected.
In Gurugram, a glaucoma assessment with Dr Shibal Bhartiya includes optic nerve imaging, visual field testing, corneal thickness measurement, and a full review of your risk profile. [second opinion]
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
⭐ Helped by this article? Leave a Google review — it helps other patients find reliable eye care.
Common Myths About Glaucoma
Most common myth about glaucoma is that it causes pain or obvious vision loss, but early glaucoma is often silent and progresses slowly. Regular eye examinations are important because glaucoma damage can occur long before symptoms become noticeable. Patients who believe they would notice symptoms, that only older people are affected, or that treatment means surgery are the patients who present late. Here is what is true, explains Dr Shibal Bhartiya.
Glaucoma affects over 12 million people in India. The majority do not know they have it. Part of the reason is the disease itself: silent, slow, and peripheral. But part of the reason is misinformation that creates false reassurance at precisely the moment awareness matters most.
Eight Glaucoma Myths That Cost People Their Vision
Myth
What the Evidence Shows
Glaucoma only affects the elderly.
While risk rises with age, glaucoma can occur at any age. Juvenile glaucoma affects teenagers. Primary open angle glaucoma is well documented in patients in their 30s and 40s, particularly in South Asian populations with high myopia or family history.
I would know if I had glaucoma — my vision is fine.
Glaucoma destroys peripheral vision first. Central vision — what you use to read and recognise faces — is preserved until very late in the disease. The brain compensates for peripheral loss so effectively that patients can lose 40% of their optic nerve before noticing anything.
Glaucoma always causes high eye pressure.
Normal tension glaucoma — where the optic nerve is damaged despite normal IOP — accounts for 30–40% of glaucoma in India. A normal pressure reading does not mean your optic nerve is safe.
Glaucoma means I will go blind.
Glaucoma diagnosed and treated early is very unlikely to cause blindness. Most patients with well-managed glaucoma retain functional vision for life. The blindness associated with glaucoma is almost always the result of late detection or inadequate treatment.
Glaucoma treatment means surgery.
The majority of glaucoma patients are managed with eye drops alone for many years. Laser procedures (SLT) are used when drops are insufficient or poorly tolerated. Surgery is reserved for cases where other treatments fail or where IOP needs to be lowered substantially.
Once I start glaucoma drops, I am on them forever.
Treatment duration depends on the stage of disease, IOP response, and patient factors. Some patients transition from drops to laser. Some achieve adequate control with laser alone. Surgical treatment can reduce or eliminate drop dependence. Your specialist reviews this regularly.
Glaucoma runs in my family but I feel fine, so I must be fine.
Family history of glaucoma increases your personal risk four to nine times. Feeling fine is expected — glaucoma is asymptomatic. A first-degree relative with glaucoma is the single strongest indication for annual specialist screening, regardless of how well you feel.
Glaucoma eye drops are just for reducing pressure — they have no other effect.
Glaucoma drops significantly affect the eye surface, causing dry eye, redness, and allergic reactions in many patients. Some systemic drops affect heart rate and blood pressure. Your specialist needs to know your full medical history and all medications before prescribing.
Frequently Asked Questions
Is There a Cure for Glaucoma?
There is no cure for glaucoma in the sense of restoring damaged nerve tissue. The optic nerve fibres lost to glaucoma do not regenerate. Treatment halts or slows progression — it does not reverse what has already been lost. This is why early detection is the single most important determinant of outcome.
Can I Check My Own Eye Pressure at Home?
Home tonometers are available and improving, but they are not a substitute for specialist monitoring. IOP is one variable in glaucoma management. Optic nerve appearance, visual field status, and nerve fibre layer thickness are equally or more important — none of which a home device measures. Home monitoring may have a role as a supplement to specialist care, not a replacement for it.
How Often Do I Need to See a Glaucoma Specialist?
This depends on your disease stage and stability. Newly diagnosed or unstable patients are typically reviewed every three to four months. Stable patients with well-controlled IOP and no progression may be reviewed every six to twelve months. Your schedule is set by your specialist and should not be deferred because you feel well.
Does Glaucoma Affect Both Eyes Equally?
Glaucoma is often asymmetric — it begins in one eye before the other and progresses at different rates. This asymmetry is one reason patients do not notice it. The better eye compensates for the worse eye. By the time both eyes are significantly affected, the window for prevention has often closed in the first eye.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Dry eye disease and glaucoma often occur together, especially because some glaucoma eye drops can affect the tear film and make symptoms like burning, irritation, watering, or fluctuating vision worse. Early diagnosis and treatment of both conditions can improve comfort and help protect long-term vision.
Glaucoma and dry eye disease occur together more often than chance alone explains. If your eyes burn, sting, or feel gritty while you are on glaucoma drops, you are not imagining it. This combination is common, clinically important, and often undertreated.
Studies consistently show that 40 to 60 percent of glaucoma patients meet diagnostic criteria for dry eye disease. The reverse is also true: people with moderate to severe dry eye carry a higher risk of developing glaucoma-related damage. These are not coincidental companions. They share biological mechanisms, and each condition can quietly worsen the other.
Why Does Dry Eye Develop in Glaucoma Patients?
The preservative problem
Most glaucoma eye drops contain benzalkonium chloride (BAK) as a preservative. BAK is effective at keeping the bottle sterile, but it is toxic to the cells of the ocular surface. It disrupts the tear film, damages goblet cells (the cells that produce the mucin layer of your tears), and triggers chronic inflammation.
Patients who use two or three glaucoma drops daily — each containing BAK — are exposing their eyes to this preservative four, six, or more times every day. Over months and years, the cumulative damage is significant. The conjunctiva becomes inflamed, the cornea loses its smooth optical surface, and the eyes feel perpetually uncomfortable.
This is not a rare side effect. It is an expected biological consequence of long-term BAK exposure, and it is one of the most underrecognised sources of glaucoma-related suffering.
Pre-existing risk
Dry eye disease is more common in the same demographic groups that develop glaucoma: older adults, women after menopause, and people with autoimmune conditions. Many patients arrive at a glaucoma diagnosis already carrying a degree of ocular surface disease. Adding BAK-containing drops to a compromised surface accelerates the damage.
Reduced blink rate
Glaucoma patients and patients with dry eye often share a common modern risk factor: prolonged screen use. Reduced blink rate during screen time is one of the fastest-growing contributors to evaporative dry eye, and it worsens the tolerance to topical medications.
Why Does This Overlap Matter Clinically?
Medication adherence
Dry eye makes glaucoma drops uncomfortable. Burning, stinging, and a sense of grittiness after instillation are among the most common reasons patients quietly reduce their drop frequency or stop altogether. This is rational behaviour in response to pain — but the result is uncontrolled intraocular pressure and silent glaucoma progression.
Treating dry eye is not a cosmetic afterthought. It is a strategy for protecting adherence, which protects the optic nerve.
Diagnostic accuracy
Dry eye causes variable intraocular pressure readings. Epithelial irregularity from a damaged ocular surface can affect tonometry (pressure measurement) and cause artificially high or variable readings. This creates noise in the data your glaucoma specialist depends on.
Similarly, a poor ocular surface causes artefacts in OCT scans and visual field tests. Blurring from unstable tear film produces dips and losses in visual field testing that mimic glaucoma progression. Distinguishing true nerve damage from tear-film artefact requires a clinician who is looking for both.
Quality of life
Glaucoma itself does not hurt and often produces no symptoms until late. But the treatment — the drops — can make patients miserable. Chronic ocular surface pain, light sensitivity, and fluctuating vision are quality-of-life burdens that patients often accept as inevitable. They are not inevitable.
How Do We Assess This in the Clinic?
A comprehensive evaluation for a glaucoma patient with ocular surface complaints includes:
Tear film assessment: Tear breakup time (TBUT) measures how quickly your tear film breaks apart after a blink. In dry eye, this is shortened.
Ocular surface staining: Fluorescein and lissamine green dyes reveal damaged cells on the cornea and conjunctiva.
Meibomian gland evaluation: Most dry eye in glaucoma patients is evaporative, caused by dysfunction of the oil-producing meibomian glands at the lid margins.
Symptom questionnaires: Validated tools like OSDI (Ocular Surface Disease Index) capture the patient experience beyond what the slit lamp shows.
Review of the current drop regimen: How many drops, which preservatives, how many times daily.
What Are the Management Options?
Switching to preservative-free formulations
This is often the single most impactful intervention. Preservative-free glaucoma drops deliver the same intraocular pressure-lowering effect without the chronic ocular surface toxicity. Multiple classes of glaucoma medication are now available in preservative-free formats: prostaglandin analogues, beta-blockers, carbonic anhydrase inhibitors, and fixed-dose combinations.
The transition requires some planning — not all formulations are available in preservative-free versions in every market, and cost is a factor — but for patients with documented ocular surface disease, this is a clinically justified switch that most guidelines now support.
Fixed-dose combination drops
Instead of using two bottles separately (each with its own preservative load), a fixed-dose combination delivers two active ingredients in one drop. This halves the number of preservative exposures per day. For patients who genuinely need two active agents, this is a practical step even before moving to preservative-free options.
Treating the dry eye directly
Ocular surface disease responds to targeted treatment. The approach depends on the type and severity:
Artificial tears: Lubricating drops, preferably preservative-free, used consistently throughout the day. These dilute residual BAK, stabilise the tear film, and reduce surface friction.
Warm compresses and lid hygiene: For meibomian gland dysfunction, daily warm compress application followed by gentle lid massage improves the quality of the oily tear layer.
Omega-3 supplementation: Good evidence supports dietary omega-3 fatty acids for meibomian gland function and tear quality.
Anti-inflammatory therapy: Topical cyclosporine (Restasis, Ikervis) or lifitegrast addresses the inflammatory cycle that perpetuates chronic dry eye. In patients with significant ocular surface inflammation, this can be transformative.
Punctal plugs: Small silicone plugs inserted into the tear drainage points slow the drainage of natural tears, keeping the eye surface better hydrated.
Laser and surgical IOP control
For some patients, reducing or eliminating the need for topical drops altogether is the right goal. Selective laser trabeculoplasty (SLT) can lower IOP without any drops. For more advanced glaucoma, surgical options including minimally invasive glaucoma surgery (MIGS) and trabeculectomy may reduce drop burden significantly. When a patient’s ocular surface is severely compromised by long-term drop use, a surgical discussion is worth having.
A Note on Sequence and Timing
When a patient presents with both conditions, the sequence of assessment matters. Dry eye can artificially distort IOP readings and OCT quality. I prefer to stabilise the ocular surface first — or at least treat both simultaneously — so that subsequent glaucoma monitoring data is reliable. A visual field test performed through an unstable tear film is not a trustworthy test.
What Should You Tell Your Doctor?
If you are being treated for glaucoma and your eyes feel uncomfortable, please say so explicitly. Many patients assume irritation is part of the package and do not raise it. Your doctor needs to know:
Which symptoms bother you most (burning, grittiness, blurred vision, light sensitivity)
Whether symptoms are worse at certain times of day or after drop instillation
Whether you have ever reduced or skipped your drops because of discomfort
Whether you use a screen for extended hours daily
This information changes the clinical approach. It does not make you a difficult patient — it makes your care more precise.
Frequently Asked Questions
Can glaucoma drops cause dry eye?
Yes. Most glaucoma drops contain benzalkonium chloride, a preservative that damages the ocular surface over time. Long-term exposure causes inflammation, goblet cell loss, and dry eye disease. Switching to preservative-free formulations often brings significant relief.
Do I have to choose between treating my glaucoma and treating my dry eye?
No. Both conditions can and should be managed simultaneously. In many cases, treating dry eye actively improves the tolerability of glaucoma drops and supports adherence to treatment, which protects the optic nerve.
Are preservative-free glaucoma drops as effective as regular drops?
Yes. The active ingredient is the same. The preservative is only there to keep the bottle sterile between uses. Preservative-free formulations use single-dose units instead, delivering the same intraocular pressure-lowering effect without the surface toxicity.
Can dry eye affect my glaucoma test results?
Yes. An unstable tear film causes variable IOP readings and artefacts in visual field and OCT testing. This is one reason a thorough ocular surface assessment is part of comprehensive glaucoma care.
I use three different glaucoma drops. Is that a problem for my eyes?
Three separate bottles often means three doses of BAK per application. This is a significant preservative load. A conversation about fixed-dose combinations or preservative-free alternatives is worth having with your glaucoma specialist.
Is laser treatment an option if my eyes cannot tolerate drops?
Yes. Selective laser trabeculoplasty (SLT) can lower IOP and reduce dependence on drops. For patients whose ocular surface disease is severe and driven by drop toxicity, reducing the drop burden through laser or surgery is a clinically sound strategy.
Internal Linking Architecture Statement
This page is part of the Glaucoma Hub hub. Read about our full approach to glaucoma diagnosis, monitoring, and treatment. Please also read our Dry Eye Hub. Here’s another heartening patient story: Tired of glaucoma eyedrops.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.