| Most common myth about glaucoma is that it causes pain or obvious vision loss, but early glaucoma is often silent and progresses slowly. Regular eye examinations are important because glaucoma damage can occur long before symptoms become noticeable. Patients who believe they would notice symptoms, that only older people are affected, or that treatment means surgery are the patients who present late. Here is what is true, explains Dr Shibal Bhartiya. |
Glaucoma affects over 12 million people in India. The majority do not know they have it. Part of the reason is the disease itself: silent, slow, and peripheral. But part of the reason is misinformation that creates false reassurance at precisely the moment awareness matters most.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Eight Glaucoma Myths That Cost People Their Vision
| Myth | What the Evidence Shows |
| Glaucoma only affects the elderly. | While risk rises with age, glaucoma can occur at any age. Juvenile glaucoma affects teenagers. Primary open angle glaucoma is well documented in patients in their 30s and 40s, particularly in South Asian populations with high myopia or family history. |
| I would know if I had glaucoma — my vision is fine. | Glaucoma destroys peripheral vision first. Central vision — what you use to read and recognise faces — is preserved until very late in the disease. The brain compensates for peripheral loss so effectively that patients can lose 40% of their optic nerve before noticing anything. |
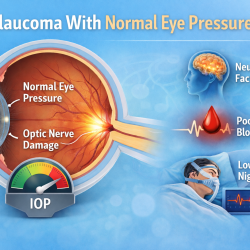
| Glaucoma always causes high eye pressure. | Normal tension glaucoma — where the optic nerve is damaged despite normal IOP — accounts for 30–40% of glaucoma in India. A normal pressure reading does not mean your optic nerve is safe. |
| Glaucoma means I will go blind. | Glaucoma diagnosed and treated early is very unlikely to cause blindness. Most patients with well-managed glaucoma retain functional vision for life. The blindness associated with glaucoma is almost always the result of late detection or inadequate treatment. |
| Glaucoma treatment means surgery. | The majority of glaucoma patients are managed with eye drops alone for many years. Laser procedures (SLT) are used when drops are insufficient or poorly tolerated. Surgery is reserved for cases where other treatments fail or where IOP needs to be lowered substantially. |
| Once I start glaucoma drops, I am on them forever. | Treatment duration depends on the stage of disease, IOP response, and patient factors. Some patients transition from drops to laser. Some achieve adequate control with laser alone. Surgical treatment can reduce or eliminate drop dependence. Your specialist reviews this regularly. |
| Glaucoma runs in my family but I feel fine, so I must be fine. | Family history of glaucoma increases your personal risk four to nine times. Feeling fine is expected — glaucoma is asymptomatic. A first-degree relative with glaucoma is the single strongest indication for annual specialist screening, regardless of how well you feel. |
| Glaucoma eye drops are just for reducing pressure — they have no other effect. | Glaucoma drops significantly affect the eye surface, causing dry eye, redness, and allergic reactions in many patients. Some systemic drops affect heart rate and blood pressure. Your specialist needs to know your full medical history and all medications before prescribing. |
Frequently Asked Questions
Is There a Cure for Glaucoma?
There is no cure for glaucoma in the sense of restoring damaged nerve tissue. The optic nerve fibres lost to glaucoma do not regenerate. Treatment halts or slows progression — it does not reverse what has already been lost. This is why early detection is the single most important determinant of outcome.
Can I Check My Own Eye Pressure at Home?
Home tonometers are available and improving, but they are not a substitute for specialist monitoring. IOP is one variable in glaucoma management. Optic nerve appearance, visual field status, and nerve fibre layer thickness are equally or more important — none of which a home device measures. Home monitoring may have a role as a supplement to specialist care, not a replacement for it.
How Often Do I Need to See a Glaucoma Specialist?
This depends on your disease stage and stability. Newly diagnosed or unstable patients are typically reviewed every three to four months. Stable patients with well-controlled IOP and no progression may be reviewed every six to twelve months. Your schedule is set by your specialist and should not be deferred because you feel well.
Does Glaucoma Affect Both Eyes Equally?
Glaucoma is often asymmetric — it begins in one eye before the other and progresses at different rates. This asymmetry is one reason patients do not notice it. The better eye compensates for the worse eye. By the time both eyes are significantly affected, the window for prevention has often closed in the first eye.
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
1500+ Five Star Patient Reviews Google Business Profile
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma
Read her research on PubMed | Google Scholar | ResearchGate | ORCID
Upload your reports for a structured review.| www.drshibalbhartiya.com | +91 88826 38735
Leave a review on Google