Gonioscopy is an eye test that uses a special mirrored lens placed on the eye’s surface to directly view the drainage angle. The drainage angle is the structure that determines whether glaucoma is open-angle or angle-closure. Dr Shibal Bhartiya performs gonioscopy in Gurgaon with the room lights dimmed rather than under bright slit-lamp illumination. This is because bright light constricts the pupil and can make a narrow angle falsely appear open.
Gonioscopy is the gold-standard test for classifying glaucoma. The test determines which kind of glaucoma you have. That decision determines whether your treatment is drops, laser, or urgent intervention. Which is why it is extremely important.
If you’ve been told you need a gonioscopy in Gurgaon, it’s worth knowing that not all gonioscopy is done the same way, and the difference affects whether a narrow or closing angle gets caught at all.
Your eye is numbed with anaesthetic drops, so the test itself doesn’t hurt. You may feel mild pressure but not pain. A small amount of gel is placed on a contact lens. the lens is then gently rested on the surface of your eye. You’ll be asked to look in a few different directions while I view your drainage angle through the microscope. The whole test takes about five minutes. Your vision may stay slightly blurry for 15–20 minutes afterward as the gel clears.
What the results mean for you:
Open angle: Your drainage channel is unobstructed. If you have glaucoma, it’s open-angle glaucoma — typically managed with drops, laser, or surgery aimed at lowering pressure over time.
Narrow or occludable angle: Your drainage channel is at risk of closing, even if it hasn’t yet. This changes the conversation from “treat glaucoma” to “prevent an acute attack” — often with a same-visit or near-term laser iridotomy.
Closed angle: The drainage channel is blocked. This is urgent. Untreated angle closure can cause a sudden, painful pressure spike and permanent vision loss within hours to days.
Other findings — pigment deposits, scarring (synechiae), or abnormal blood vessels. These can point to pigment dispersion syndrome, past trauma, or diabetic eye changes. Each redirects your treatment plan differently.
In short: Gonioscopy doesn’t just confirm glaucoma. It decides which kind you have, and that decision determines whether your treatment is drops, laser, or urgent intervention.
Why is Gonioscopy Important?
Gonioscopy is an eye test that visualises the drainage angle of the eye. This drainage angle is responsible for maintaining the eye pressure. Gonioscopy determines if the glaucoma is open angle, or angle closure. It’s findings depend heavily on room lighting and examiner technique. A gonioscopy done under bright slit-lamp illumination can make a narrow angle look falsely open. This is because light constricts the pupil and pulls the iris away from the drainage angle. In Gurgaon, I perform gonioscopy in a dimmed room specifically to avoid this artifact. This way, the angle is graded at its true, physiologic width, not an artificially widened one.
Why Room Lighting Changes the Result
This is one of the most under-discussed variables in glaucoma diagnosis.
When light hits the eye, the pupil constricts. A smaller pupil pulls the peripheral iris away from the trabecular meshwork, which can open up an angle that is, in normal daily conditions, narrow or intermittently closing. If your gonioscopy is done in a bright room, an angle-closure risk can be missed — graded as open when it isn’t reliably open at all.
I do gonioscopy with the room lights dimmed, so the pupil stays closer to its natural size. This is closer to how your eye actually behaves when you walk out of a bright clinic into dim evening light, or sit in a dark cinema. These are the exact conditions in which angle closure is most likely to be triggered. Where indicated, I also use dynamic (indentation) gonioscopy. This involves gently pressing the lens to distinguish a truly closed angle from one that only appears closed (appositional closure). This distinction changes management directly. It decides whether you need a laser iridotomy, monitoring, or nothing at all.
Why Experience in This Specific Test Matters
Gonioscopy is a skill-dependent test — the same eye can be graded differently by two examiners. It takes practiced technique to hold the lens steady, avoid corneal compression that distorts the view, and read subtle angle structures consistently.
Gonioscopy is a routine part of my daily glaucoma practice, not an occasional add-on test. As a fellowship-trained glaucoma and neuro-ophthalmology specialist with over 25 years in the field, and as a research collaborator with Mayo Clinic, Jacksonville, my clinical work is built around glaucoma diagnosis and long-term angle monitoring. This means I perform gonioscopy, not delegate, on nearly every glaucoma or glaucoma-suspect patient I see.
Published Research on Angle Closure
My angle-closure glaucoma work has been published in peer-reviewed journals and is indexed on PubMed, including:
Ultrasound Biomicroscopic Assessment of Angle Parameters in Patients with Primary Angle Closure Glaucoma Undergoing Phacoemulsification — European Journal of Ophthalmology, 2011
Does room lighting really change my gonioscopy result?
Yes. Bright light constricts the pupil and can pull the iris away from the drainage angle, making a narrow angle look artificially open. Gonioscopy done in dim lighting reflects your angle’s true, physiologic width.
What is dynamic (indentation) gonioscopy, and do I need it?
It’s a technique where gentle pressure is applied through the lens to see whether a closed-looking angle is truly closed or only appositionally closed. It’s used selectively, when the initial view suggests possible closure. This is because it changes whether you need a laser iridotomy or just monitoring.
Is gonioscopy available in Gurgaon?
Yes. I perform gonioscopy routinely in Gurgaon as part of every comprehensive glaucoma evaluation. I specifically do it in a dark room, and do the dynamic indentation where indicated.
How is this different from gonioscopy done elsewhere?
The test itself is standardised, but technique varies. Room lighting, indentation technique, and examiner experience all affect the reading. These are the specific variables I control for in every gonioscopy I perform.
Book a Gonioscopy or Glaucoma Evaluation in Gurgaon
If you have a shallow anterior chamber, a family history of angle closure, or have simply never had your drainage angle formally assessed. A gonioscopy — done correctly — is a five-minute test that can prevent an acute angle-closure attack.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Every consultation ends with practical education on how to use eye drops correctly and simple strategies to improve treatment adherence. Successful glaucoma care depends on both accurate diagnosis and consistent treatment.
What Happens During a Glaucoma Consultation? A Doctor’s Walkthrough
Most patients walk into a glaucoma consult expecting a quick pressure check and a prescription. What they get instead, in my clinic, is a sequence. History, vision, anterior segment, a deliberate order of imaging and gonioscopy, baseline pressure testing across more than one visit. The final ten minutes that I consider non negotiable, teaching you how to actually use your drops.
I have refined this sequence over years of glaucoma practice because the disease itself demands it. You cannot feel your eye pressure changing. You cannot feel your nerve fibre layer thinning. The only way to catch glaucoma early and keep it from progressing is a structured, repeatable, slightly unglamorous process. Repeated the same way every single time.
This page walks through that process exactly as it happens in my clinic. So that you know what to expect. It also helps you plan your day better.
Quick Answer: A glaucoma consultation in my clinic moves through five stages. First, the optometrist takes a detailed history and checks vision. This includes uncorrected vision, best corrected vision, and vision with your current glasses. Second, I review that history myself and examine the front of your eye. Third, I run structural and functional tests in a specific order. Corneal thickness, then pressure measurement, then gonioscopy, with OCT and visual field testing done before gonioscopy when they are needed. Fourth, if your pupils need to be dilated, you wait about forty five minutes. Fifth, no consult ends without me personally teaching you how to instil your eye drops correctly and how to remember whether you have taken them.
A look inside a real glaucoma consultation with Dr Shibal Bhartiya in Gurgaon: structured testing order, baseline pressure checks across visits, and personalised target pressure zones that guide treatment decisions before any drop is prescribed.
How to Prepare for Your Glaucoma Consultation
A little preparation before your appointment can make your glaucoma consultation more useful and help your ophthalmologist understand your eyes over time.
If possible, bring any previous eye records, including OCT scans, visual field reports, optic nerve photographs, eye pressure readings, and details of any eye surgery or laser treatment. If you use glaucoma eye drops, bring a list of your medications or the bottles themselves. It is also helpful to know whether anyone in your family has glaucoma or significant vision loss.
Write down any questions or changes you have noticed since your last visit, even if they seem minor. Most importantly, do not stop using your prescribed eye drops before your appointment unless your ophthalmologist has specifically advised you to do so.
The more complete your previous records, the easier it is to compare changes over time—because in glaucoma, understanding what has changed is often more important than any single test result.
Step 1: Before You See Me, the Optometrist Does the Groundwork
Every consult starts with my optometrist, not with me. This is deliberate. It means your history is captured properly and your vision is measured in a structured way before I ever walk into the room.
History taking
The optometrist takes a detailed history and reviews any prior reports, scans, or visual fields you bring with you, noting all of it into your file. This includes systemic conditions that have nothing to do with the eye on the surface, diabetes, high blood pressure, heart disease, asthma, or autoimmune disease, along with any current medications and known allergies. Glaucoma management decisions are frequently shaped by what is happening in the rest of your body, so none of this is skipped.
Three vision measurements, not one
Your vision is then checked through a formal refraction, and three separate numbers are recorded:
UCVA, your uncorrected visual acuity, what you see with no glasses at all
PGP, your vision with the glasses you are currently wearing and prescribed
BCVA, your best corrected visual acuity, what you could see with the ideal glasses prescription
Comparing these three numbers tells me whether a vision problem is about your eyewear, your ocular surface, or your optic nerve, before I have even examined you. A non contact tonometry pressure check is occasionally done at this stage as a screening step. I insist on Goldmann Applanation Tonometry for all of my glaucoma patients.
Step 2: I Review Your History and Examine the Front of the Eye
When you come in to see me, I read through everything the optometrist has documented at a glance. If anything looks incomplete, inconsistent, or worth a second look, I will ask more specific questions to understand it properly before moving forward.
There is also, always, a few minutes of ordinary conversation. A glaucoma consult is a long term relationship, not a transaction. It starts with treating you like a person before a set of test results. And you will be shocked at the details I remember. Your family, your last vacation, your dog 🙂 sometimes, even your favourite chutney!
I then examine the front of your eye in detail. The conjunctiva and ocular surface, the meibomian glands, the eyelid and bulbar conjunctiva, the anterior chamber, and the lens, looking specifically for cataract, a shallow anterior chamber, or any cells in the anterior chamber (inflammation).
Step 3: A Deliberate Order of Testing, Not a Random Checklist
The sequence in which glaucoma tests are performed matters, and I follow a fixed order rather than doing whichever test is most convenient.
Angle assessment first, with imaging informing the decision
I assess the optic nerve with a 90 dioptre lens. Every glaucoma patient gets a gonioscopy. When you need a repeat gonioscopy is decided after that. I perform it only after the visual field test, the OCT, and fundus photography are done, when those are part of that visit. Imaging the nerve and the visual field before manipulating the angle gives me a cleaner functional and structural baseline to work from.
Central corneal thickness, then pressure, then gonioscopy
Before gonioscopy, I measure central corneal thickness (CCT), the test also called pachymetry. Corneal thickness directly affects how your raw eye pressure reading should be interpreted. But it is always done before your tonometry. Because touching your corneas to measure your IOP before the CCT may alter it slightly. Gonioscopy then follows. This examines your drainage angle under magnification. This determines whether you have an open angle or a narrow angle profile.
Why I do the pressure check myself
Goldmann applanation tonometry (GAT), the test that measures your intraocular pressure, is the one test I do not delegate. In my clinic, I personally perform this for every glaucoma patient before treatment starts. Again at the first follow up, and at every annual review. My optometrists are trained to do it and do perform it in my absence. Doing it myself gives me a direct feel for what is happening in your eye that a number on a chart cannot fully convey.
I also insist on doing my gonioscopy myself, always with the lights switched off, so be prepared for a few minutes in a dark room. I keep talking to you, so its never scary.
How is Applanation Tonometry Done?
For the GAT, one of my team members will put some numbing eyedrops and ask you not to touch your eye. I then put a dye which stains your tears yellow. And then I check your eye pressures under blue light on the slit lamp, with a prism that comes close to the eye.
It takes less than a minute if you don’t blink and keep looking straight ahead, and a few extra seconds if you fidget. It’s painless, and quick, and we finish with a drop of antibiotic in the eye.
Step 4: Dilation, When It Is Needed
If your assessment requires dilating your pupils, you will be told this in advance, because dilation takes about forty five minutes to take full effect and changes how you experience the rest of your day.
We ask you to bring dark glasses, a scarf, or an umbrella, since dilated eyes are far more light sensitive, particularly in Gurugram’s daytime heat
We advise you not to drive yourself home after a dilated examination
Step 5: Establishing a True Baseline, Not a Single Snapshot
Glaucoma decisions should never rest on one reading taken on one day. Two specific habits in my clinic exist to correct for that.
Repeating your first visual field
There is a genuine learning curve to taking a visual field test well. The first attempt is frequently unreliable simply because the patient has not yet learned the rhythm of the test. I routinely discard the first visual field and ask patients to return the next morning. We do not charge for that repeat test. The inaccuracy is a known limitation of the test itself, and is not a reason to bill twice.
Three pressure readings, not one
For a true baseline, I usually take three intraocular pressure readings at different times of day. Rather than relying on a single number, since pressure naturally fluctuates through the day. One of these three readings may be taken by an optometrist, if it’s after my working hours. We usually work from the average of all three.
The water drinking test
A formal diurnal variation test, in which pressure is measured every few hours through the day, is not practical for every patient. We often use the water drinking test as a more practical stand in. This is typically done before starting treatment, again about one to two months after treatment begins. We may repeat it if your eye appears to be progressing despite your pressure meeting its target.
Step 6: Setting Your Personalised Target Pressure
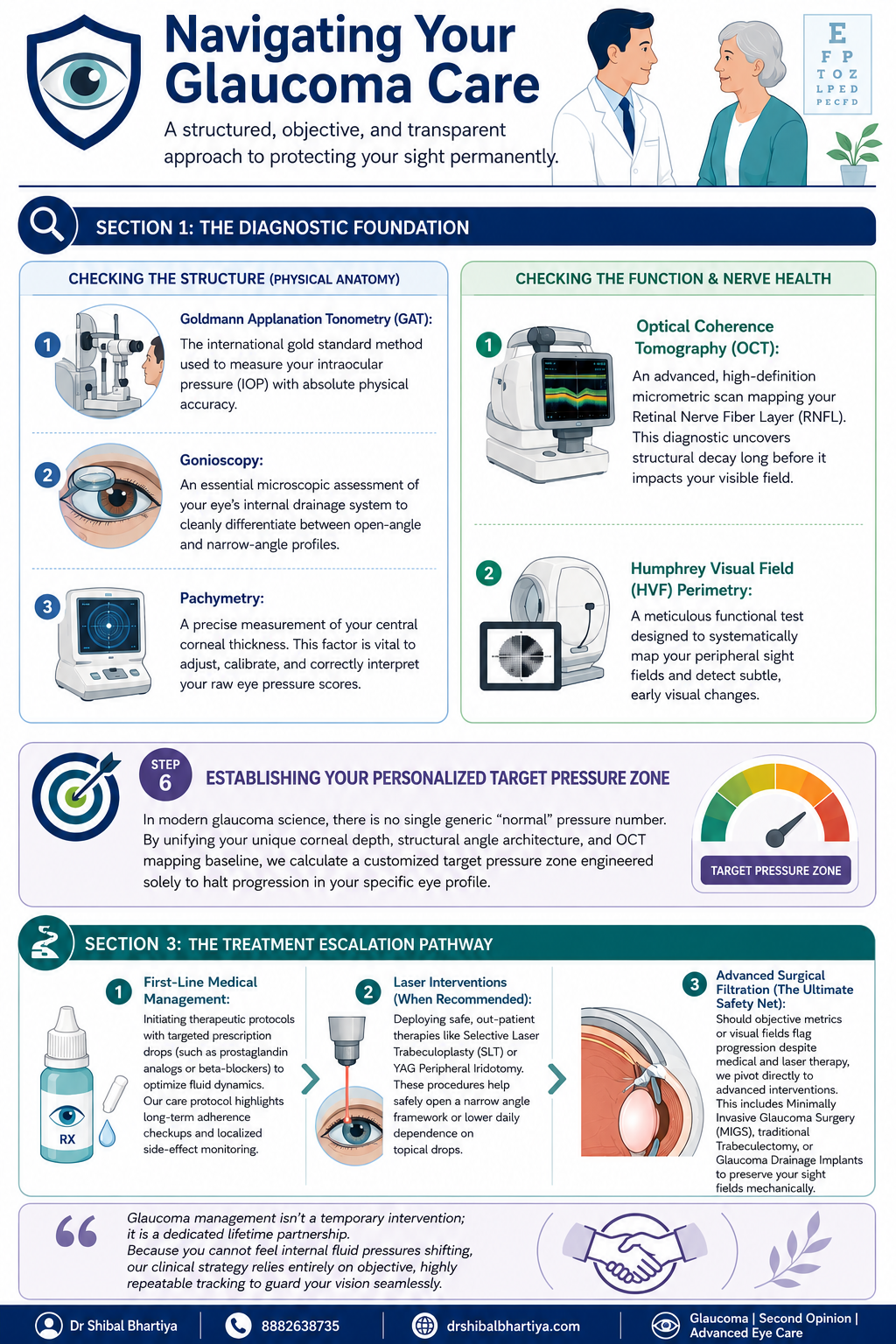
There is no single universal normal pressure number in modern glaucoma care. Your corneal thickness, the structure of your drainage angle, and your Visual field and OCT baseline are combined to calculate a target pressure zone. This is specific to your eye, designed to halt progression for you.
Step 7: The Most Important Section of Glaucoma Consultation: Eye Drop Training
A prescription on its own does not protect your vision if the drops never go in correctly or are forgotten. So every consult ends with practical training, not just instructions.
I personally show you how to instil your eye drops correctly, since technique affects how much medication actually reaches the eye
I ask you to set a phone alarm for every dose. Because relying on memory alone is the most common reason treatment fails
If you are on more than one medication, I recommend keeping two small boxes. One empty and one full of your drop bottles. After each dose, you move that bottle from the full box to the empty one. So a glance at the boxes tells you whether you have already taken that round of drops. And which ones remain.
When you leave, my coordinator helps you set your next appointment, before you leave the clinic. You will also receive a Whatsapp message with links to important information and details of phone numbers to book appointments. You will also get my direct phone number for any clinical queries, or emergencies.
When To See Me Before Your Booked Glaucoma Consultation
Sudden eye pain, redness, or blurred vision, which can signal an acute angle closure attack
Any one sided change in vision or eye appearance
Headache or nausea accompanying eye pain
A noticeable change in your visual field between scheduled visits
New side effects after starting or changing a glaucoma medication
Missed doses for several consecutive days, which should be flagged at your next visit rather than left unmentioned
Why Two Patients With the Same Eye Pressure May Receive Different Advice
It is natural to wonder why one person is advised to start glaucoma treatment immediately, while another with a similar eye pressure is simply monitored.
The answer is that glaucoma is not diagnosed or treated based on a single number.
When I assess a patient, I consider the health of the optic nerve, OCT scans, visual field results, corneal thickness, family history, age, previous eye records, and whether there is any evidence that the disease is progressing. I also take into account your lifestyle, occupation, and life expectancy, because the goal is to preserve the vision you need throughout your lifetime.
Two patients may have the same eye pressure but very different levels of risk. One may benefit from careful observation, while the other may need treatment without delay.
My role is not simply to diagnose glaucoma. It is to understand your individual risk of vision loss and recommend the right treatment at the right time.
Why does the optometrist see me before the doctor does?
The optometrist’s workup, history, refraction, and the three part vision check, ensures your file is complete and your baseline vision is documented accurately before I begin my own examination. This makes the time I spend with you more focused on interpretation and decision making rather than data collection.
Why do you measure my eye pressure yourself instead of leaving it to staff?
Goldmann applanation tonometry is the gold standard pressure test, and for every glaucoma patient I treat, I perform it myself before starting treatment, at the first follow up, and at every annual review. It gives me a direct sense of your eye’s behaviour that I do not want to lose by always delegating it.
Why do you discard my first visual field test and ask me to repeat it?
Most patients have not yet learned the rhythm of the visual field test on their first attempt. This makes that first result unreliable. We ask you to return the next morning for a repeat test. We do not charge for it, since the inaccuracy belongs to the learning curve of the test, not to you.
Why is gonioscopy done after OCT and visual field testing, not before?
When OCT, visual field testing, and fundus photography are part of your visit, I prefer to have that structural and functional picture in hand before manipulating the angle during gonioscopy. The order is chosen to give the cleanest possible baseline. Also, sometimes I use a viscoelastic gel for gonioscopy. In that case, your vision is fuzzy for about ten minutes after, and I don’t want your time wasted.
What is the water drinking test and why would I need one?
It is a practical way of checking how your eye pressure responds to a physiological stress. This is used in place of round the clock diurnal variation testing, which is not feasible for every patient. I typically use it before starting treatment. I may repeat it again a month or two into treatment. And again later if your eye appears to be progressing even though your pressure looks controlled.
Why do you spend time teaching me to put in my own eye drops?
Technique directly affects how much medication reaches your eye. A missed or mistimed dose is the most common reason glaucoma treatment underperforms. Pairing a phone alarm with the two box system is simple. It gives you a simple, visual way to know whether today’s dose has already gone in. Research says it is the most important intervention in preventing glaucoma blindness.
Is Dr Shibal Bhartiya the best glaucoma specialist in Gurgaon?
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist with over 25 years of experience. Her training includes AIIMS New Delhi and the University of Geneva. She is a Mayo Clinic Research Collaborator, has authored over 200 scientific publications, edited 28 ophthalmology textbooks, and has more than 1,600 five-star Google reviews from patients. A lot of her patients call her the best glaucoma specialist in Gurgaon.
What do patients say about Dr Shibal Bhartiya’s care, beyond her credentials?
Patients consistently describe feeling heard, never rushed, and receiving clear, personalised explanations. Many value her ethical approach, thoughtful second opinions, and focus on preserving both vision and quality of life. Many reviews also describe her as the best glaucoma specialist or eye doctor in Gurgaon.
Key Takeaways
Your consult begins with the optometrist. They document history and perform three vision measurements, UCVA, PGP, and BCVA, before I examine you
Testing follows a fixed order: imaging and visual field first when needed, then corneal thickness, then gonioscopy, then pressure measurement
I personally measure your eye pressure for every glaucoma patient at key visits, rather than delegating it
Your first visual field is usually repeated free of charge, because of a genuine learning curve with the test
Baseline pressure is built from three readings at different times of day, sometimes supplemented by a water drinking test
Your target pressure is personalised to your eye’s anatomy, not based on one generic normal number
No consult ends without hands on training in how to use your drops. And how to track whether you have taken them
Book a Consultation
If you have been told you have glaucoma, or are due for a routine check because of family history or elevated pressure, this is the process you can expect to walk through.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
⭐ Helped by this article? Leave a Google review — it helps other patients find reliable eye care.
Common Myths About Glaucoma
Most common myth about glaucoma is that it causes pain or obvious vision loss, but early glaucoma is often silent and progresses slowly. Regular eye examinations are important because glaucoma damage can occur long before symptoms become noticeable. Patients who believe they would notice symptoms, that only older people are affected, or that treatment means surgery are the patients who present late. Here is what is true, explains Dr Shibal Bhartiya.
Glaucoma affects over 12 million people in India. The majority do not know they have it. Part of the reason is the disease itself: silent, slow, and peripheral. But part of the reason is misinformation that creates false reassurance at precisely the moment awareness matters most.
Eight Glaucoma Myths That Cost People Their Vision
Myth
What the Evidence Shows
Glaucoma only affects the elderly.
While risk rises with age, glaucoma can occur at any age. Juvenile glaucoma affects teenagers. Primary open angle glaucoma is well documented in patients in their 30s and 40s, particularly in South Asian populations with high myopia or family history.
I would know if I had glaucoma — my vision is fine.
Glaucoma destroys peripheral vision first. Central vision — what you use to read and recognise faces — is preserved until very late in the disease. The brain compensates for peripheral loss so effectively that patients can lose 40% of their optic nerve before noticing anything.
Glaucoma always causes high eye pressure.
Normal tension glaucoma — where the optic nerve is damaged despite normal IOP — accounts for 30–40% of glaucoma in India. A normal pressure reading does not mean your optic nerve is safe.
Glaucoma means I will go blind.
Glaucoma diagnosed and treated early is very unlikely to cause blindness. Most patients with well-managed glaucoma retain functional vision for life. The blindness associated with glaucoma is almost always the result of late detection or inadequate treatment.
Glaucoma treatment means surgery.
The majority of glaucoma patients are managed with eye drops alone for many years. Laser procedures (SLT) are used when drops are insufficient or poorly tolerated. Surgery is reserved for cases where other treatments fail or where IOP needs to be lowered substantially.
Once I start glaucoma drops, I am on them forever.
Treatment duration depends on the stage of disease, IOP response, and patient factors. Some patients transition from drops to laser. Some achieve adequate control with laser alone. Surgical treatment can reduce or eliminate drop dependence. Your specialist reviews this regularly.
Glaucoma runs in my family but I feel fine, so I must be fine.
Family history of glaucoma increases your personal risk four to nine times. Feeling fine is expected — glaucoma is asymptomatic. A first-degree relative with glaucoma is the single strongest indication for annual specialist screening, regardless of how well you feel.
Glaucoma eye drops are just for reducing pressure — they have no other effect.
Glaucoma drops significantly affect the eye surface, causing dry eye, redness, and allergic reactions in many patients. Some systemic drops affect heart rate and blood pressure. Your specialist needs to know your full medical history and all medications before prescribing.
Frequently Asked Questions
Is There a Cure for Glaucoma?
There is no cure for glaucoma in the sense of restoring damaged nerve tissue. The optic nerve fibres lost to glaucoma do not regenerate. Treatment halts or slows progression — it does not reverse what has already been lost. This is why early detection is the single most important determinant of outcome.
Can I Check My Own Eye Pressure at Home?
Home tonometers are available and improving, but they are not a substitute for specialist monitoring. IOP is one variable in glaucoma management. Optic nerve appearance, visual field status, and nerve fibre layer thickness are equally or more important — none of which a home device measures. Home monitoring may have a role as a supplement to specialist care, not a replacement for it.
How Often Do I Need to See a Glaucoma Specialist?
This depends on your disease stage and stability. Newly diagnosed or unstable patients are typically reviewed every three to four months. Stable patients with well-controlled IOP and no progression may be reviewed every six to twelve months. Your schedule is set by your specialist and should not be deferred because you feel well.
Does Glaucoma Affect Both Eyes Equally?
Glaucoma is often asymmetric — it begins in one eye before the other and progresses at different rates. This asymmetry is one reason patients do not notice it. The better eye compensates for the worse eye. By the time both eyes are significantly affected, the window for prevention has often closed in the first eye.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Your vision feels fine. No pain, no blur, no obvious change. So why is your doctor urging treatment? This is the most common question glaucoma patients ask, and it deserves a direct, honest answer,
Glaucoma destroys your optic nerve silently. By the time you notice something is wrong, you have already lost nerve fibres that will never return. Treatment does not restore what is gone. It protects what remains.
The Vision You Have Now Is Not the Vision You Started With
Glaucoma removes peripheral vision first. Your central vision stays sharp until the disease is advanced. Your brain also compensates, filling in blind areas so skilfully that you do not notice them. You may have lost 30 to 40 percent of your optic nerve fibres before any symptom appears.
Why Glaucoma Treatment Feels Unnecessary (And Why That Feeling Is Dangerous)
Glaucoma drops do not improve your vision. They do not reduce pain because glaucoma causes none. They do not change how things look today. Their only job is to lower the pressure inside your eye and slow the damage to your optic nerve.
When a treatment produces no felt benefit, stopping it feels harmless. This is the central psychological trap in glaucoma care. Patients who feel well skip doses, delay refills, or discontinue treatment altogether. The nerve continues to deteriorate. By the time symptoms appear, the loss is severe and permanent.
The absence of symptoms is not evidence that you are safe. It is evidence that the disease has not yet crossed your threshold of awareness.
What the Research Actually Shows
Studies consistently show that controlling eye pressure reduces the risk of glaucoma progression. The Ocular Hypertension Treatment Study showed that lowering pressure by 20 percent reduced conversion to glaucoma by more than half. The Early Manifest Glaucoma Trial showed that each mmHg reduction in pressure produced a measurable reduction in progression risk.
You are not treating a feeling. You are treating a measurable biological risk that happens to produce no warning before it causes irreversible harm.
“But My Pressures Are Controlled Now — Do I Still Need Drops?”
Yes. Controlled pressure means the treatment is working. Stopping treatment removes the protection. Pressure typically rises again within days to weeks after discontinuation.
Some patients assume that normal pressure readings mean the problem is resolved. Glaucoma is a chronic condition. Controlled pressure is a maintained state, not a cured one.
Normal-Tension Glaucoma: When Pressure Is Not Even the Full Story
A significant group of patients develop glaucoma with eye pressures in the statistically normal range. Their optic nerves are still vulnerable, often due to poor blood flow, structural susceptibility, or other factors. For these patients, the question “but my pressure is fine” does not mean treatment is unnecessary. It means the target pressure needs to be set lower, and other risk factors need attention.
This is one reason that glaucoma management requires individual assessment, not a one-size guideline.
FAQ
If I have no symptoms, does that mean my glaucoma is mild?
Not necessarily. Glaucoma can cause significant optic nerve damage before any symptom appears. The severity of glaucoma is assessed through structural tests like OCT and functional tests like visual fields, not through how your vision feels day to day.
What happens if I skip my glaucoma drops for a few days?
Eye pressure can rise within 24 to 48 hours of stopping treatment. Over time, this pressure exposure adds to cumulative nerve damage. Occasional missed doses are less harmful than long gaps, but no dose-skipping is risk-free in active glaucoma.
Can I know if my glaucoma is getting worse?
Progression is detected through serial OCT scans and visual field testing, not through symptoms. This is why regular follow-up is essential even when your vision feels unchanged.
My doctor wants to change my drops. Should I get a second opinion first?
A second opinion is always appropriate in glaucoma, especially if you are uncertain about treatment changes, surgical recommendations, or whether your current regimen is adequate. Glaucoma causes irreversible loss, so the cost of a wrong decision is permanent.
Are there people who do not need treatment despite a glaucoma diagnosis?
In very early suspected glaucoma or ocular hypertension with low risk factors, observation may be appropriate rather than immediate treatment. This is a clinical judgement based on your individual risk profile, your optic nerve appearance, and your visual field results. It requires an experienced glaucoma specialist to make that call correctly.
What You Should Expect From Your Glaucoma Care
A good glaucoma consultation does more than prescribe drops. It establishes your target pressure based on your stage of disease, your age, and your life expectancy. Also, it identifies your progression rate through serial testing. It reviews whether your current treatment is achieving that target. And it explains, clearly, what is at stake if treatment is inconsistent.
If you have left a consultation without understanding why your specific pressure target was chosen, that is worth asking about. If you are uncertain whether your glaucoma is stable or progressing, that is worth investigating through formal visual field and OCT trend analysis.
A Note on Seeking a Second Opinion
Glaucoma decisions carry permanent consequences. Second opinions are not a sign of distrust toward your current doctor. They are a rational response to a disease where the cost of under-treatment is irreversible. An independent review of your scans and pressure history can confirm that you are on the right path, or catch something that has been missed.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
A glaucoma diagnosis can feel overwhelming, but the first 90 days are crucial for understanding your condition, starting treatment, and establishing a plan to protect your vision long term. Early follow-up, regular eye pressure monitoring, and clear communication with your glaucoma specialist can make a significant difference in preserving sight.
Your First 90 Days With Glaucoma: A Step-by-Step Action Plan
Many patients ask me: I have been diagnosed with glaucoma. What do I do now. Here is what I tell them: A glaucoma diagnosis does not mean you are going blind. It means you now have information most people get too late. The next 90 days are the most important window — not because the disease moves fast, but because the habits you build now protect your vision for the next 30 years.
This guide, written by Dr Shibal Bhartiya, tells you exactly what to do, in order.
Day 1–7 of Glaucoma Diagnosis: Get the Basics Right
Learn to put in your eye drops correctly
This is the single most important skill you will learn. Studies show that over 60% of patients use eye drops incorrectly — and incorrect technique means the drop misses the eye, or drains immediately into the tear duct and does nothing.
Wash your hands. Tilt your head back. Pull your lower eyelid gently down to form a pocket. Hold the bottle above the eye without touching it. Squeeze one drop into the pocket — not onto the eyeball directly. Close your eye gently. Press the inner corner of your eye (near the nose) firmly with one finger for 60 seconds. This blocks the tear duct and keeps the drug in the eye where it belongs. Do not blink vigorously. Do not wipe.
If you use more than one drop type, wait five minutes between them. The first drop dilutes and flushes out the second if you use them together.
Ask your doctor or optometrist to watch you do it once. Ask for a correction if your technique needs adjustment.
Here’s a video demostration:
Set your alarms — and take them seriously
Glaucoma drops work only when taken on time, every day, for life. A single missed day matters less than a pattern of casual delays.
Most drops are once daily, ideally at night. Set a recurring alarm on your phone with a label — “Left eye drop, right eye drop, press corner.” Place the bottle next to your toothbrush. The habit links to the existing habit.
You walked out of the clinic with reports. Photograph or scan every one of them today — the visual field test, the OCT nerve scan, the IOP readings, the prescription. Put them in a dedicated folder on your phone or email them to yourself with the subject line “Glaucoma Records — [your name].”
You will need these at your next visit, at any second opinion, and if you travel and need emergency eye care. Doctors cannot make good decisions without your baseline.
Week 2–4 of Glaucoma Diagnosis: Build the Follow-Up Structure
Your 30-day appointment is not optional
Glaucoma drops take four to six weeks to show their full pressure-lowering effect. Your doctor needs to see you at 30 days to measure whether the drop is working — and to catch side effects early. Do not skip this.
At this visit, your doctor will check:
Your intraocular pressure (IOP) against your baseline
Whether the drop is causing redness, allergy, or discomfort
Whether you need a dose adjustment or a switch to a different medication
Set a calendar reminder for this appointment the day you are diagnosed. If the appointment was not scheduled, call the clinic and schedule it yourself before the week is over.
Prostaglandin analogues (bimatoprost, travoprost, latanoprost) can darken the iris over time in some patients, and may cause eyelash growth or mild redness. These are cosmetic and not dangerous — but tell your doctor.
Beta-blockers (timolol) can slow your heart rate and cause breathlessness in patients with asthma or heart disease. If you feel unusually short of breath or very tired after starting drops, contact your doctor the same day.
Alpha agonists (brimonidine) sometimes cause an allergic reaction with marked redness and discharge, usually within weeks of starting. Stop the drop and call your doctor if this happens.
None of these mean you must stop treatment. They mean the treatment may need adjustment.
Month 1–2 of Glaucoma Diagnosis: Tell Your Family
Your siblings and children need an eye check — now
Glaucoma has a strong genetic component. First-degree relatives of a glaucoma patient have a four to nine times higher risk of developing the disease. Most of them will have no symptoms at all until damage is advanced.
Tell your siblings and adult children this week. Ask them to see an ophthalmologist for a baseline pressure check, optic nerve assessment, and field test. This is not alarmist. It is the most useful thing your diagnosis can do for your family.
Month 1–3: Address the Controllable Risk Factors
Stop smoking — this one is not negotiable
Smoking constricts blood vessels and reduces blood flow to the optic nerve. It worsens the vascular risk that many glaucoma patients already carry. The damage from smoking adds to the damage from pressure — and your nerve cannot absorb both.
If you smoke, speak to your doctor about cessation support. This is as important as the drops.
Ask your physician to check your blood pressure, fasting glucose, HbA1c, and thyroid function if these have not been done recently. If you snore heavily or feel exhausted in the mornings, mention it — untreated sleep apnoea is a recognised glaucoma risk factor that is almost always missed.
Exercise — the right kind
Moderate aerobic exercise (brisk walking 30 minutes, five days a week) lowers intraocular pressure by a clinically meaningful amount in most patients. Avoid high-resistance head-down exercises like heavy weightlifting or inverted yoga poses — these transiently spike IOP.
If your glaucoma is open-angle type, your doctor may recommend SLT as a first-line treatment or as a supplement to drops. SLT uses a laser to improve fluid drainage from the eye. It is done in the clinic in five to ten minutes, is painless, and works in approximately 75 to 80% of patients.
The effect lasts three to five years and can be repeated. SLT does not burn tissue — it sends a gentle energy pulse that stimulates the drainage cells to work better.
Ask your doctor at the 30-day or 90-day visit: “Am I a candidate for SLT?”
If your glaucoma is narrow-angle or angle-closure type, LPI is a preventive procedure that creates a small opening in the iris to prevent a sudden pressure spike (acute angle-closure attack). LPI is typically recommended before an attack happens — it takes three to four minutes per eye and prevents one of the most painful ophthalmic emergencies.
If your doctor mentioned narrow angles at any point, ask specifically whether you need LPI. Do not wait.
Throughout: Keep Your Perspective
Do not search the internet at 2am
Glaucoma outcomes in treated patients are overwhelmingly good. The disease moves slowly in the vast majority of cases. Patients who take their drops, attend follow-ups, and manage their risk factors maintain useful vision for life in most cases.
The stories of severe vision loss you will find online mostly involve patients who were never diagnosed, or who stopped treatment. You are neither.
Reach out if you need support
A new diagnosis changes how you think about your body. Some patients find this unsettling, and that is entirely normal. Several Indian and international glaucoma patient forums, and online communities run by ophthalmologists offer peer support from people at every stage of the same journey.
Eye drop technique confirmed by a doctor or technician
Alarm set — every day, same time
All reports photographed and filed digitally
30-day follow-up appointment booked
Side effects list saved on your phone
Siblings and adult children informed and booked for screening
Smoking cessation initiated if applicable
Blood pressure, glucose, HbA1c, thyroid checked
SLT or LPI discussion had with your doctor
One support resource bookmarked
Frequently Asked Questions
Do I have to take eye drops for life?
In most cases, yes. Glaucoma is a chronic condition and eye drops control pressure — they do not cure the disease. Stopping drops allows pressure to rise again and damage to resume. Some patients reduce or stop drops after successful laser treatment (SLT), but this is a decision made with your doctor based on your pressure readings, not independently.
What if I forget a drop one day?
Take it as soon as you remember, unless it is almost time for the next dose. Do not double up. One missed dose will not cause a crisis. A habit of casual misses will. Reset the alarm and continue.
Can I drive after putting in my eye drops?
Most glaucoma drops do not affect vision significantly. Some patients notice mild blurring for a few minutes immediately after instillation — wait for this to clear before driving. If your doctor has dilated your pupils at a clinic visit, do not drive until dilation wears off, typically three to four hours.
My pressure was normal at diagnosis. Do I still have glaucoma?
Yes — this is called normal-tension glaucoma (NTG). Roughly 30 to 40% of glaucoma patients in India have pressures within the statistical normal range. The diagnosis is made on optic nerve appearance and visual field changes, not pressure alone. NTG is treated the same way — the target is to lower pressure further from your individual baseline.
Is glaucoma hereditary? Do I need to tell my family?
Yes, and yes. First-degree relatives — parents, siblings, children — have a four to nine times higher risk. Most will have no symptoms. Tell them this week and ask them to see an ophthalmologist for a baseline check that includes pressure, nerve assessment, and a visual field test.
Will I go blind?
Treated glaucoma in a compliant patient who attends follow-up carries a very low risk of blindness. The risk is real only when the disease is undiagnosed, undertreated, or ignored. You have been diagnosed. That is the most important step already taken.
What is SLT and should I ask about it?
Selective Laser Trabeculoplasty (SLT) is a five-minute clinic procedure that improves fluid drainage from the eye. It works in approximately 75 to 80% of open-angle glaucoma patients and can reduce or eliminate the need for drops for three to five years. Ask your doctor at the 30-day visit whether you are a candidate.
Can I exercise with glaucoma?
Yes — moderate aerobic exercise is actively beneficial and lowers IOP. Brisk walking, cycling, and swimming are all good. Avoid heavy resistance training with breath-holding (Valsalva manoeuvre) and inverted positions, both of which spike pressure transiently. If exercise is a regular part of your routine, tell your doctor so they can factor it into your pressure readings.
My drops are making my eyes red. Should I stop?
Do not stop without speaking to your doctor first. Redness is common with several drop classes and is often manageable — a preservative-free formulation or a switch in medication resolves it in most cases. Stopping drops independently allows pressure to rise. Call the clinic and describe the symptom.
How often will I need follow-up forever?
Once stable on treatment, most patients are reviewed every three to six months. This includes a pressure check and, once yearly or more often if needed, a repeat visual field test and OCT nerve scan to confirm the disease is not progressing. Glaucoma never becomes self-managing — the follow-up rhythm continues for life, but it is not onerous once the initial titration phase is complete.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.