
Optic nerve damage is diagnosed early using tests like OCT scans and visual field testing to detect subtle structural and…
Tag: family history glaucoma screening
Can Routine Eye Tests Miss Glaucoma?
Routine eye tests can appear normal in early glaucoma because they measure visual clarity, not optic nerve damage or functional loss patterns. Glaucoma often develops silently, with structural damage occurring before any noticeable change in vision.
It is difficult to believe that sometimes routine eye tests miss glaucoma. Most patients diagnosed with glaucoma say the same thing:
“But I was getting regular eye check-ups.”
This question is painful, but very important. Glaucoma can exist with completely normal vision, especially in early stages.
Routine eye tests can sometimes miss early glaucoma. Not because doctors are careless, and not because patients did anything wrong, but because glaucoma is a quiet disease that often hides in plain sight.
Understanding this helps patients make calmer, better decisions, says Dr Bhartiya.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Why Routine Eye Tests Miss Glaucoma
1. Glaucoma Has No Early Symptoms
In early glaucoma, vision is usually perfect. You can read clearly, drive, and work normally while small optic-nerve fibres are already lost. This is called structural damage before functional loss.
Routine exams focused on glasses or cataract may not detect this.
2. Eye Pressure Can Be Normal
Many patients have normal-tension glaucoma. So a quick pressure check does not rule out disease. Moreover, your eye pressure fluctuates through the day. This is called diurnal variation of IOP.
Eye pressure is only one part of glaucoma evaluation, and moreover, one single reading is not adequate representation of what happens through the day. This is one of the reasons why routine eye tests miss glaucoma.
3. Single Tests Can Mislead
Glaucoma diagnosis needs a combination of:
• optic nerve examination
• OCT imaging
• visual field testing
• corneal thickness
• angle examination (gonioscopy / ASOCT)
• family history
• comparison over time
Looking at one test alone can miss subtle disease, or cause unnecessary fear.
If your OCT shows red areas or your field test is flagged, do not panic. Many of these findings need careful interpretation before they mean anything definitive.
4. The Brain Compensates
Patients adapt quietly. They stop night driving. Read more slowly. Walk carefully in dim light. the vision charts and power of glasses remain normal.
Routine exams rarely ask about these subtle changes.
5. Follow-Up Drift
Documentation of clinical findings is often inadequate. Patients are told to return after one year. Some don’t. Others just get their power of glasses checked. Some change doctors, others lose records. Sometimes reports are not compared carefully. Small progression is thus missed.
This is a systems problem, not a patient mistake.
How Often Do Routine Eye Tests Miss Glaucoma?
More often than most people realise. Population-based studies in India, including large community studies in South India, have shown that glaucoma frequently remains undetected. This is true even in people who had already undergone cataract surgery. Cataract surgery improves vision but does not rule out glaucoma.
Across India, it is estimated that around 90% of glaucoma cases remain undiagnosed.
Even in developed countries, glaucoma diagnosis is difficult. Studies show both under-diagnosis and over-diagnosis are common. This is because glaucoma cannot be diagnosed from one test alone. It requires interpretation of patterns over time.
These numbers remind us that glaucoma is a subtle disease, not a simple one.
What a Proper Glaucoma Check Should Include
A structured glaucoma evaluation includes:
• optic nerve assessment
• OCT nerve fibre analysis
• visual field testing
• corneal thickness measurement
• angle examination
• risk stratification
• comparison over time
Because glaucoma is a slow disease, continuity of care matters more than a single visit.
Who Should Be Checked Even If Vision Is Normal
• Age above 40
• Family history of glaucoma
• High myopia
• Diabetes or hypertension
• Long-term steroid use
• Women caring for families who delay their own care
These groups need structured follow-up. This does not mean everyone with these risk factors needs glaucoma investigations. It means they need a comprehensive eye evaluation, with special focus on glaucoma.
Who Needs Glaucoma Investigations, and When?
Glaucoma testing is recommended whenever risk factors are present, even if vision feels normal. This includes people with a suspicious optic nerve appearance, ocular hypertension (eye pressure above 21 mmHg), thin corneas, a strong family history of glaucoma, or previous eye injury. Patients with high myopia, diabetes, or long-term steroid use also need evaluation. Because glaucoma is usually silent early, investigations should begin when these risk factors are first detected and be repeated at intervals based on individual risk so that subtle progression is not missed.
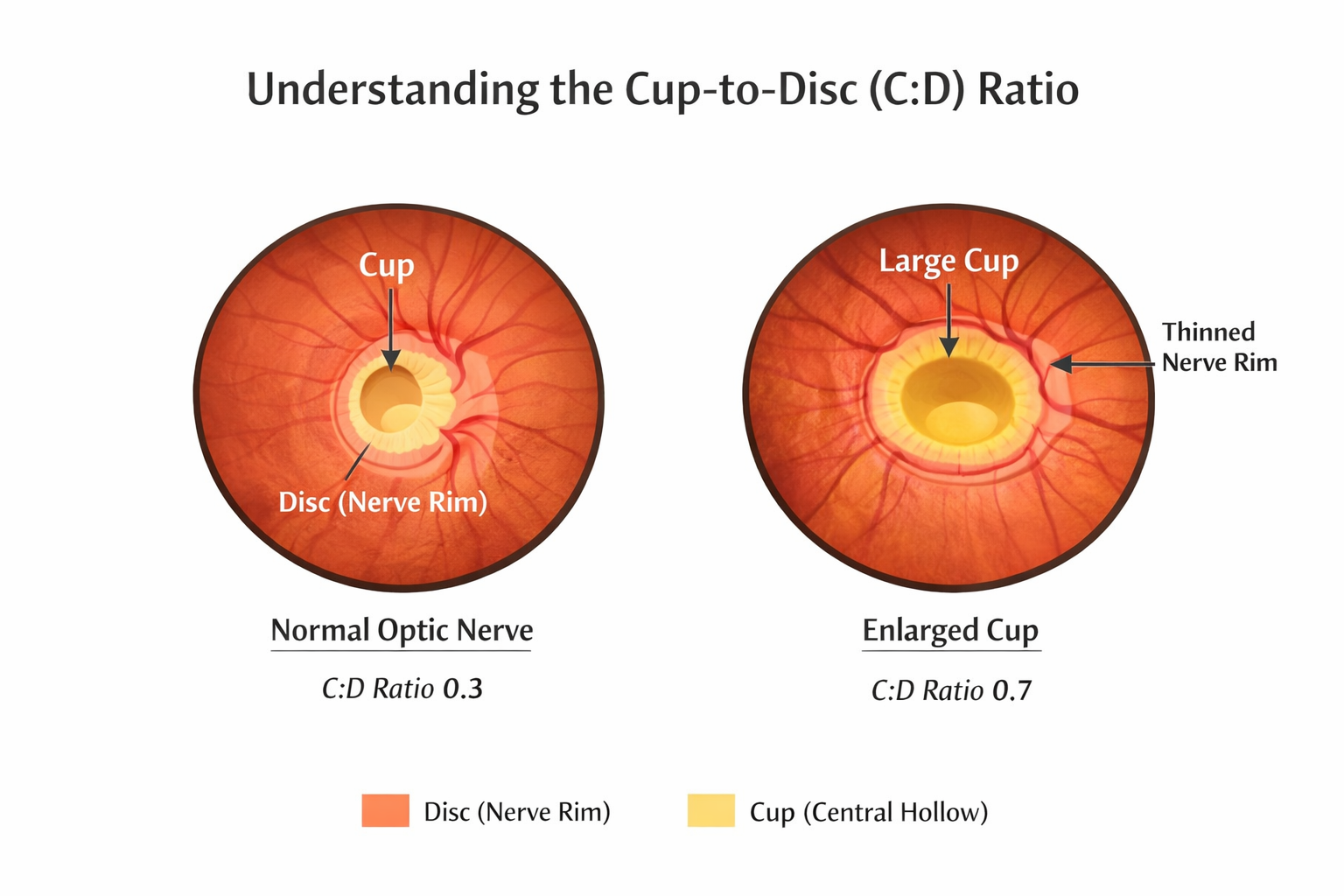
What Does “C:D Ratio” Mean?
The optic nerve has a small central hollow called the cup, surrounded by nerve tissue called the disc.
The cup-to-disc ratio (C:D) compares the size of this hollow to the whole optic nerve.
A C:D ratio greater than about 0.5, especially if it is increasing or the different between the two eyes is more than 0.2, can suggest possible nerve fibre loss and may need glaucoma testing.
However, C:D size varies naturally between people. Some individuals have large cups but healthy nerves. This is why the C:D ratio must always be interpreted along with OCT scans, visual field testing, and comparison over time. Numbers alone do not diagnose glaucoma, patterns do.
What Does “IOP > 21 mmHg” Mean?
IOP stands for intra-ocular pressure, the pressure inside the eye.
Pressures above 21 mmHg are considered higher than average. Ocular hypertension is defined as high eye pressures with no fucntional or structural damage to the optic nerve.
Not everyone with high pressure develops glaucoma, and some people develop glaucoma with normal pressure. But raised pressure increases risk and requires careful monitoring and sometimes treatment to protect the optic nerve.
Because glaucoma is usually invisible early, patients with ocular hypertension need structured follow-up even if vision is clear.
The Bigger Lesson
Early, consistent care prevents regret later. In glaucoma, we are not protecting eyesight today. We are protecting your vision for the rest of your life.
Healthcare systems are built around treating visible disease. Glaucoma is invisible early. So routine eye tests miss glaucoma. This is not anyone’s fault. But it means patients must ask questions and doctors must think long-term.
When a Second Opinion Helps
A second opinion is not about doubting your doctor. It is about understanding your own risk clearly.
Because glaucoma is subtle, a structured second opinion can be useful when:
• Reports are confusing
• Advised surgery suddenly
• Multiple drops started without explanation
• OCT and visual field results disagree
• Strong family history of glaucoma/ glaucoma blindness
A calm review of tests over time often clarifies risk.
The Importance of Serial Comparison
The most important glaucoma test is comparison.
We compare:
• OCT over years
• visual fields over years
• optic nerve photos
Progression becomes visible only in hindsight. That is why follow-up matters.
Common Misinterpretations
• Red OCT areas in high myopia
• Field defects from cataract
• Machine artefacts
• Ignoring early thinning
Patients should not panic. Or be falsely reassured, without explanation. A structured interpretation is essential to clarify, and stratify, risk.
My Approach
My approach to glaucoma evaluation begins with reviewing all prior reports in sequence: not just the most recent one. I look for patterns across OCT, visual field, and optic nerve imaging over time, because glaucoma progression only becomes visible when tests are compared, not read in isolation. Every patient receives a written risk summary and a clear explanation of what needs monitoring and why. I review all reports systematically with attention to long-term risk.
Closing Thought
Seeing clearly is not the same as seeing safely. In glaucoma, we are not protecting eyesight today. We are protecting your eyes for the rest of your life.
Early, consistent care matters more than dramatic late treatment.
Most patients who contact me are not yet sure they have glaucoma. That is exactly the right time to ask.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma
Related Reading
Get an Online Glaucoma Consult
Why Do I Need a Visual Field Test?
Understanding Your OCT Report in Glaucoma
Visual Field and OCT: Structure & Function Correlation
Understanding Glaucoma
Understanding Glaucoma: A Complete Patient Guide
Understanding Glaucoma: A Complete Patient Guide, has been written by Dr Shibal Bhartiya, glaucoma specialist in Gurgaon, and last reviewed in April, 2026. Glaucoma is one of the leading causes of irreversible blindness in the world. In India, it affects an estimated 12 million people. Most of them do not know they have it.
This is the defining challenge of glaucoma. It does not announce itself. It causes no pain. It takes vision slowly, quietly, and permanently, starting at the edges, where you are least likely to notice.
This guide explains what glaucoma is, how it develops, who is at risk, how it is diagnosed, and how it is treated. It is written by Dr Bhartiya for patients who want to understand their disease clearly — and for those who want to know whether they should be screened.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Key Facts
- Glaucoma is a disease of the optic nerve — not simply a disease of eye pressure.
- It causes no pain and no early symptoms in most cases.
- Vision loss from glaucoma is irreversible. What is lost cannot be restored.
- Early detection through regular screening is the most powerful protection.
- Glaucoma is treatable. Most patients retain useful vision with early diagnosis and consistent care.
- Family history is one of the strongest risk factors. First-degree relatives need regular screening.
What Is Glaucoma?
Glaucoma is a group of eye diseases that damage the optic nerve. The optic nerve connects the eye to the brain. It carries the visual signals that create everything we see.
When the optic nerve is damaged, those signals are lost. The damage is permanent. No treatment can restore vision that glaucoma has already taken.
In most forms of glaucoma, raised intraocular pressure (IOP) — the pressure inside the eye — is the main driver of optic nerve damage. Fluid called aqueous humour constantly circulates inside the eye. When this fluid cannot drain properly, pressure builds up. Over time, that pressure damages the optic nerve fibres.
But glaucoma is not simply a pressure disease. Some patients develop optic nerve damage with entirely normal pressure. Others have high pressure for years without developing glaucoma. Pressure is important — but it is one factor in a more complex picture.
Why Glaucoma Is Called the Silent Thief of Sight
The optic nerve contains over one million nerve fibres. Glaucoma damages these fibres gradually. The nerve has a large functional reserve — it can lose up to 40% of its fibres before central vision is affected.
The first vision to be lost is peripheral — the edges of the visual field. This loss is so gradual that most patients do not notice it. The brain compensates. The other eye fills in gaps. By the time a patient realises something is wrong, the disease is often advanced.
There is no pain, and no redness in the early stages. There is no sudden change. Just quiet, steady, invisible loss.
This is why screening matters more than waiting for symptoms. In glaucoma, symptoms mean the disease is already advanced.
Types of Glaucoma
Glaucoma is not a single disease. It is a family of conditions. Understanding which type you have determines how it is managed.
Primary Open Angle Glaucoma (POAG)
This is the most common type. The drainage angle of the eye is open, but the drainage system works too slowly. Pressure rises gradually. Damage develops over years — often without any symptoms until late in the disease. POAG is the type most people mean when they say ‘glaucoma’.
Normal Tension Glaucoma (NTG)
In this type, optic nerve damage occurs despite normal eye pressure. Blood flow to the optic nerve, structural vulnerability, and other factors are involved. Normal tension glaucoma is often missed because doctors and patients assume that normal pressure means no glaucoma risk.
Angle Closure Glaucoma (Narrow Angle / PACG)
In this type, the drainage angle is physically blocked or too narrow. It can occur suddenly — an acute angle closure attack causes severe eye pain, blurred vision, redness, and nausea. But more often, it develops slowly and silently, just like open angle glaucoma. Angle closure is more common in people of Asian origin (including Indians), in women, and in those with a plus spectacle number.
Ocular Hypertension
Eye pressure is raised, but the optic nerve shows no damage yet. This is not glaucoma — it is a risk state. Not all patients with high pressure develop glaucoma. But all need monitoring, and some need treatment.
Glaucoma Suspect
A patient is called a glaucoma suspect when one or more findings — suspicious optic nerve appearance, borderline pressure, or thin cornea — raise concern, but the diagnosis is not yet confirmed. Careful monitoring over time establishes whether glaucoma is developing.
Secondary Glaucoma
Secondary glaucoma arises as a consequence of another eye condition. Causes include pseudoexfoliation syndrome, pigment dispersion, uveitis, trauma, and steroid use. Treatment addresses both the underlying cause and the raised pressure.
Who Is at Risk of Glaucoma?
Anyone can develop glaucoma. But these factors significantly increase risk:
Family History
Glaucoma is strongly hereditary. If a parent or sibling has glaucoma, your risk is four to nine times higher than average. This is the single most actionable risk factor — it identifies who needs screening before symptoms appear. Regular family history glaucoma screening is essential for first-degree relatives.
Age
Risk rises steadily after age 40. After 60, glaucoma is significantly more common. But glaucoma can develop at any age, including in young adults and children.
Raised Eye Pressure
High intraocular pressure is the most important modifiable risk factor. But it neither confirms nor excludes glaucoma. Pressure must always be interpreted alongside optic nerve appearance, visual fields, and OCT findings.
Ethnicity
Open angle glaucoma is more common and more aggressive in people of African origin, often appearing at a younger age. Angle closure glaucoma is more prevalent in people of Asian and South Asian origin. Indian patients carry a significant burden of both types.
Refractive Error
High myopia (strong minus prescription) increases risk of open angle glaucoma. High hyperopia (plus prescription) increases risk of angle closure glaucoma.
Thin Cornea
A thin central cornea is associated with higher glaucoma risk. It also causes eye pressure to be under-read by tonometry — meaning actual pressure may be higher than measured. Corneal thickness measurement (pachymetry) is an important part of glaucoma risk assessment.
Systemic Conditions
Diabetes, cardiovascular disease, and migraine all affect blood flow to the optic nerve and increase glaucoma risk. Sleep apnoea has also been linked to optic nerve damage.
Steroid Use
Prolonged use of steroid eye drops, nasal sprays, or oral steroids can raise eye pressure and cause steroid-induced glaucoma. Patients on long-term steroids need regular eye pressure monitoring.
Early Glaucoma Symptoms: What to Watch For
In the early stages, most patients have no symptoms at all. This is not unusual. This is what understanding glaucoma means. It is the nature of the disease. When symptoms do appear, they are often subtle:
- Gradual loss of peripheral vision
- Small blind spots in the visual field
- Blurred vision
- Halos around lights, especially at night
- Frequent changes in spectacle prescription
- Difficulty adjusting between bright and dark environments
In advanced disease:
- Significant narrowing of the visual field
- Tunnel vision
- Difficulty reading or driving
Symptoms of an Acute Angle Closure Attack
Acute angle closure is a medical emergency. Seek immediate care if you experience:
- Severe eye pain
- Sudden significant blurring of vision
- Red eye
- Coloured halos around lights
- Headache, nausea, or vomiting
Most patients with glaucoma never experience an acute attack. The chronic, silent form is far more common and far more dangerous over time.
Emergency contact number: +91 9818700269 | +91 8882638735
How Is Glaucoma Diagnosed?
No single test diagnoses glaucoma. In fact, routine tests often miss glaucoma. Diagnosis requires a combination of assessments, interpreted together by a glaucoma specialist. This is why a dedicated glaucoma evaluation is different from a routine eye check. Recognising this is important for understanding glaucoma.
Eye Pressure Measurement (Tonometry)
Intraocular pressure is measured at every glaucoma appointment. The normal range is 10–21 mmHg. But normal pressure does not rule out glaucoma — and raised pressure does not confirm it. Pressure must be measured at multiple time points. It varies with time of day.
Optic Nerve Examination
The optic nerve is examined directly through a dilated pupil. A glaucoma specialist looks for cupping of the nerve, notching of the neuroretinal rim, asymmetry between the two eyes, and disc haemorrhages. This examination is the cornerstone of glaucoma diagnosis.
OCT – Optical Coherence Tomography
OCT measures the thickness of the retinal nerve fibre layer (RNFL) around the optic nerve. It detects structural damage before visual field loss appears. OCT is one of the most sensitive tools for early glaucoma detection and is essential for monitoring progression over time.
Visual Field Testing (Perimetry)
Perimetry maps the full extent of vision, central and peripheral. It detects and tracks functional loss caused by glaucoma. Serial visual fields over time are the primary tool for assessing whether glaucoma is progressing.
Gonioscopy
Gonioscopy uses a special contact lens to directly examine the drainage angle. It distinguishes open angle from angle closure glaucoma, a critical distinction because the two require different treatment. Gonioscopy is essential in every new glaucoma evaluation.
Pachymetry- Corneal Thickness
Central corneal thickness affects how accurately pressure is measured. A thin cornea causes pressure to be under-read. It is also an independent risk factor for glaucoma progression.
Why Routine Eye Tests Can Miss Glaucoma
Standard eye examinations focus on spectacle power, cataract, and retinal health. They do not routinely include gonioscopy, detailed optic nerve grading, OCT, or serial visual fields. A patient can have early glaucoma, and normal vision, and be told their eyes are completely fine at a routine check.
This is not negligence. It reflects the fact that glaucoma detection requires a dedicated, specialty-level evaluation, not a standard optometry appointment.
How Is Glaucoma Treated?
There is no cure for glaucoma. But treatment works. It lowers eye pressure and protects the optic nerve from further damage. Most patients with early diagnosis and consistent treatment retain good functional vision for life.
The goal of treatment is not to restore lost vision. It is to preserve what remains.
Eye Drops
Pressure-lowering eye drops are the most common first-line treatment. Prostaglandin analogues (latanoprost, bimatoprost, travoprost) are given once daily and are the most widely used. Other classes include beta-blockers, carbonic anhydrase inhibitors, and alpha-agonists. Some patients need combinations.
Drop adherence, using drops correctly and consistently, is the single most important factor in preventing glaucoma progression. Missing doses allows pressure to rise and damage to continue.
SLT Laser: Selective Laser Trabeculoplasty
SLT is a laser treatment that improves drainage from the eye. It is now recognised as a first-line option, equivalent to eye drops, based on the LiGHT trial. SLT is an outpatient procedure. It is repeatable. It reduces the need for long-term drops in many patients.
Laser Peripheral Iridotomy (LPI)
LPI is the primary treatment for narrow angle glaucoma and angle closure risk. A small laser opening in the iris allows fluid to bypass a blocked drainage pathway. It is an outpatient procedure performed under topical anaesthetic.
Trabeculectomy
Trabeculectomy is the gold standard surgical procedure for glaucoma. It creates a new drainage pathway — a small flap in the eye wall — allowing fluid to drain and pressure to fall significantly. It is used when drops and laser cannot achieve adequate pressure control. It is highly effective but requires careful postoperative management.
MIGS: Minimally Invasive Glaucoma Surgery
MIGS procedures improve drainage through very small incisions, with a lower risk profile than trabeculectomy. They are suitable for mild to moderate glaucoma and are often combined with cataract surgery. They offer a meaningful reduction in pressure and drops, but cannot achieve the very low pressures that trabeculectomy provides.
Glaucoma Drainage Implants
In complex or refractory cases, a small silicone tube drains fluid from the eye to a plate on its surface. Tube shunts are used when trabeculectomy has failed or is unlikely to succeed.
Observation
Not all glaucoma requires immediate treatment. In patients with very early disease, low risk of progression, and reliable follow-up, careful monitoring may be the appropriate initial approach. Observation is not inaction, it is structured, evidence-based surveillance.
Why Lifelong Monitoring Is Essential
Glaucoma is a lifelong condition. Controlled glaucoma is not cured glaucoma.
Regular monitoring continues throughout a patient’s life, even when pressure is well controlled and vision is stable. The reason is simple: glaucoma can change. Pressure can rise. Progression can resume. A bleb can scar over. A drop that worked for years can stop working.
Follow-up appointments typically include eye pressure measurement, optic nerve assessment, OCT imaging, and visual field testing. The frequency depends on the severity of disease and rate of progression.
Missing follow-up appointments is the most common reason glaucoma causes preventable vision loss.
When to Seek a Glaucoma Second Opinion
A second opinion in glaucoma is not about distrust. It is about getting clarity on a disease that is often complex, lifelong, and consequential.
Consider a structured second opinion if:
- You have been told you have glaucoma but are uncertain about the diagnosis
- You have been advised surgery and want to understand whether it is the right next step
- Your glaucoma is progressing despite treatment
- Your current treatment plan feels unclear or uncertain
- You want an independent assessment of your pressure targets and monitoring plan
- When you are anxious about the days ahead, and unable to cope
Glaucoma second opinions are particularly valuable before major surgical decisions. The best surgical decision is an informed one. Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides independent, trusted second opinions for patients seeking clarity before major treatment decisions.
Not sure about your diagnosis? You are not alone.
Many patients come to Dr Bhartiya after receiving a glaucoma diagnosis elsewhere — unsure whether to start treatment, concerned about long-term progression, or simply wanting clarity before committing to a plan.
A second opinion is not a sign of distrust. It is good medicine.
Request a Glaucoma Second Opinion →
Does Glaucoma Cause Blindness?
Glaucoma is a leading cause of irreversible blindness worldwide. But for most patients diagnosed early, the answer is no, glaucoma does not cause blindness.
The patients who go blind from glaucoma are almost always those who were diagnosed late, who did not receive appropriate treatment, or who stopped attending follow-up. With early diagnosis, correct treatment, and consistent long-term care, most patients retain functional vision for life.
Glaucoma is not a sentence. It is a manageable chronic disease, when managed.
When to Seek a Glaucoma Evaluation
You should have a dedicated glaucoma evaluation, not just a routine eye test, if:
- You are over 40 and have a first-degree relative with glaucoma
- You have been told your eye pressure is raised or borderline
- Your optic nerve has been described as suspicious
- You have a strong minus or plus spectacle power
- You have diabetes, high blood pressure, or a history of migraines
- You use steroid drops, nasal sprays, or oral steroids long-term
- You have never had a detailed optic nerve assessment
- You have noticed any loss of peripheral vision or other visual changes
Early detection is simple. The consequences of missing it are not.
Frequently Asked Questions About Glaucoma
What causes glaucoma?
Most glaucoma is caused by impaired drainage of fluid from the eye, leading to raised intraocular pressure that damages the optic nerve over time. In normal tension glaucoma, damage occurs despite normal pressure, suggesting blood flow to the nerve and structural vulnerability also play a role. Secondary glaucomas are caused by other eye conditions, medications, or systemic disease.
Is glaucoma hereditary?
Yes. Glaucoma has a strong genetic component. If a parent or sibling has glaucoma, your risk is four to nine times higher than average. Family history glaucoma screening for first-degree relatives is strongly recommended from age 40, or earlier if other risk factors are present.
Can you have glaucoma with normal eye pressure?
Yes. Normal tension glaucoma is a well-recognised condition in which the optic nerve sustains damage despite pressure within the normal range. Normal pressure does not exclude glaucoma. A proper glaucoma evaluation assesses the optic nerve directly, not just the pressure reading.
Can glaucoma be cured?
No. Glaucoma cannot be cured. The vision already lost cannot be restored. But treatment controls the disease effectively in most patients. With early diagnosis and consistent care, most patients retain useful vision throughout their lives.
What is the difference between early and advanced glaucoma?
Early glaucoma involves optic nerve damage that has not yet affected the functional visual field. Vision remains normal. Advanced glaucoma has caused significant peripheral, or in severe cases central, visual field loss. Early glaucoma can be managed to prevent progression. Advanced glaucoma requires treatment to prevent further loss.
What tests are needed to diagnose glaucoma?
A complete glaucoma evaluation includes eye pressure measurement (tonometry), optic nerve examination through dilated pupils, OCT imaging of the retinal nerve fibre layer, visual field testing (perimetry), gonioscopy to examine the drainage angle, and corneal thickness measurement (pachymetry). No single test is sufficient. Diagnosis requires all findings to be interpreted together.
How often should a glaucoma patient be seen?
This depends on the severity of disease, rate of progression, and stability of pressure control. Patients with controlled, stable early glaucoma may be seen every 6–12 months. Those with active progression, recent treatment changes, or advanced disease need more frequent monitoring, sometimes every 1–3 months.
Can glaucoma affect both eyes?
Yes. Glaucoma usually affects both eyes, though often one eye is more severely affected than the other. Each eye is assessed and managed individually. Treatment may differ between the two eyes.
Is surgery always necessary for glaucoma?
No. Most patients are managed successfully with eye drops and/or laser. Surgery is needed when drops and laser cannot achieve adequate pressure control, when disease is progressing despite treatment, or when pressure needs to be lowered significantly and sustainably to protect the optic nerve.
Where can I see a glaucoma specialist in Gurgaon?
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Clinical Director of Ophthalmology at Marengo Asia Hospitals, Sector 56, Gurugram. She offers comprehensive glaucoma evaluations, second opinions, and the full range of glaucoma treatments including laser, trabeculectomy, and MIGS. She is also a Research Collaborator with Mayo Clinic, Florida. Visit drshibalbhartiya.com or call +91 88826 38735.
Glaucoma does not need panic. It needs clarity, consistency, and the right specialist.
Early detection, thoughtful risk assessment, and steady follow-up protect vision over decades. Most patients with glaucoma live full, visually intact lives, when their disease is found early and managed well.
Explore Related Topics
This guide brings together the most important information patients need to understand glaucoma, from early detection to long-term care decisions. This page is the starting point. Each topic below has its own dedicated guide on this site:
- Glaucoma Specialist in Gurgaon
- Open Angle Glaucoma
- Narrow Angle Glaucoma
- Ocular Hypertension
- Glaucoma Surgery in Gurgaon
- Glaucoma Second Opinion
- Laser or Eye Drops for Glaucoma
- Can Glaucoma Be Cured?
- Is My Glaucoma Getting Worse?
- Glaucoma Treatment options
- MIGS: Surgical Options for Glaucoma Treatment
- Myths about Glaucoma
- Living with Glaucoma; Home environment
- Glaucoma Evaluation in Gurgaon
- Teleconsultation | Online consultation
- Glaucoma Progression Despite Eye Drops
- Do Glaucoma Patients Go Blind
- Glaucoma tests explained
- Visual Field
- OCT
- Gonioscopy
- Why so many tests for glaucoma
Diagnosed with narrow angles, angle closure, borderline eye pressure? Advised laser? A second opinion, or a structured glaucoma evaluation can provide:
- An accurate assessment of your actual risk level
- Clarity on whether treatment is necessary at this stage
- A personalised monitoring or management plan
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. This article was edited in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Her work can be accessed on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile

Glaucoma Suspect
A glaucoma suspect is someone who has a risk of developing glaucoma. This includes higher pressure in the eye, evidence of optic nerve damage or vision loss. Glaucoma can cause irreversible vision loss, and usually has no early symptoms.

Dilated Eye Exam
A dilated eye exam is a part of your comprehensive eye check. Your eye doctor checks your eye, after putting drops to make the pupils larger.