A glaucoma consultation in my clinic follows a structured five-step process. Detailed history and vision assessment, comprehensive eye examination, glaucoma-specific testing (including corneal thickness, eye pressure, gonioscopy, OCT, and visual fields when needed), pupil dilation if required, and a personalized discussion of findings.
Every consultation ends with practical education on how to use eye drops correctly and simple strategies to improve treatment adherence. Successful glaucoma care depends on both accurate diagnosis and consistent treatment.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
What Happens During a Glaucoma Consultation? A Doctor’s Walkthrough
Most patients walk into a glaucoma consult expecting a quick pressure check and a prescription. What they get instead, in my clinic, is a sequence. History, vision, anterior segment, a deliberate order of imaging and gonioscopy, baseline pressure testing across more than one visit. The final ten minutes that I consider non negotiable, teaching you how to actually use your drops.
I have refined this sequence over years of glaucoma practice because the disease itself demands it. You cannot feel your eye pressure changing. You cannot feel your nerve fibre layer thinning. The only way to catch glaucoma early and keep it from progressing is a structured, repeatable, slightly unglamorous process. Repeated the same way every single time.
This page walks through that process exactly as it happens in my clinic. So that you know what to expect. It also helps you plan your day better.
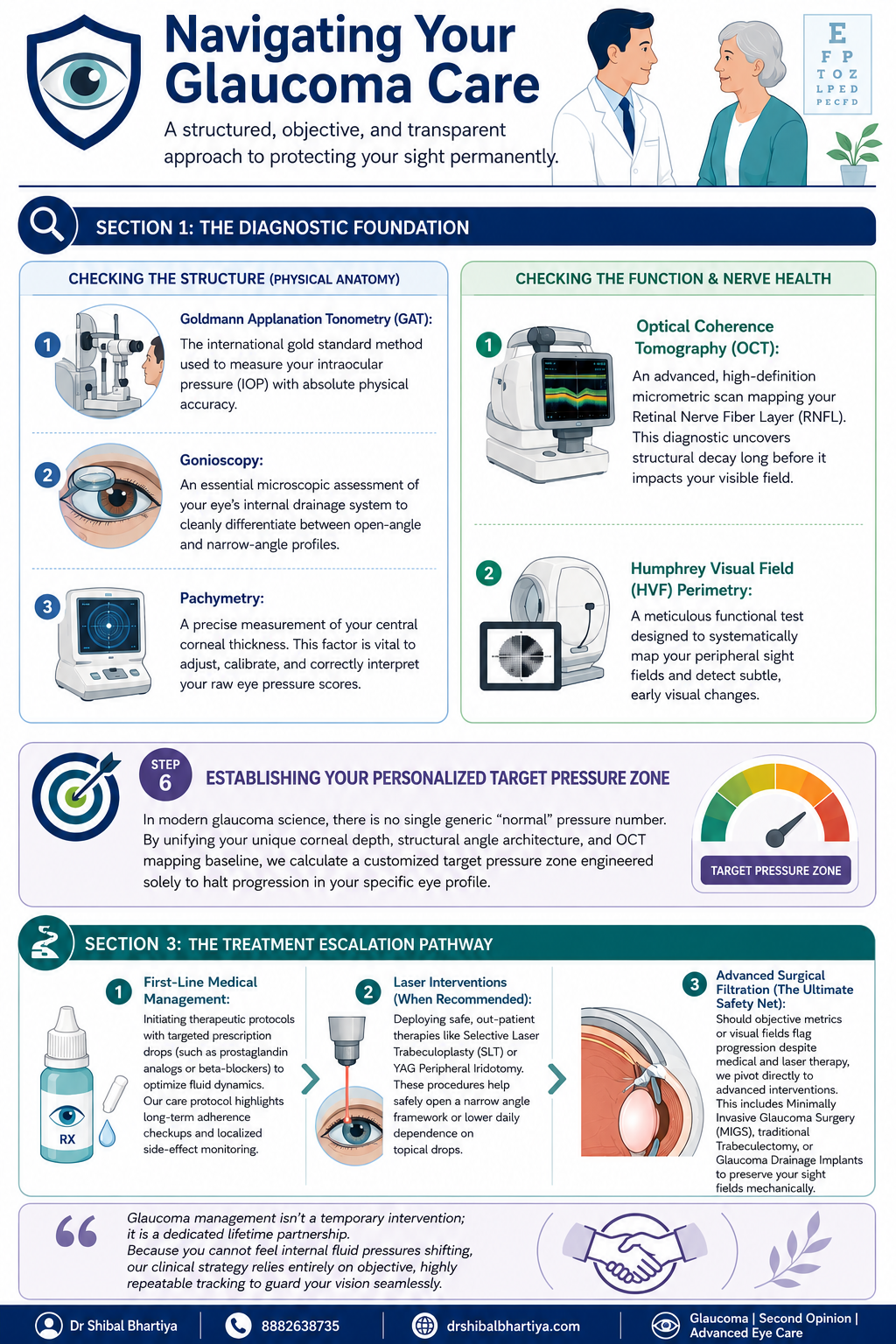
Quick Answer: A glaucoma consultation in my clinic moves through five stages. First, the optometrist takes a detailed history and checks vision. This includes uncorrected vision, best corrected vision, and vision with your current glasses. Second, I review that history myself and examine the front of your eye. Third, I run structural and functional tests in a specific order. Corneal thickness, then pressure measurement, then gonioscopy, with OCT and visual field testing done before gonioscopy when they are needed. Fourth, if your pupils need to be dilated, you wait about forty five minutes. Fifth, no consult ends without me personally teaching you how to instil your eye drops correctly and how to remember whether you have taken them.
Step 1: Before You See Me, the Optometrist Does the Groundwork
Every consult starts with my optometrist, not with me. This is deliberate. It means your history is captured properly and your vision is measured in a structured way before I ever walk into the room.
History taking
The optometrist takes a detailed history and reviews any prior reports, scans, or visual fields you bring with you, noting all of it into your file. This includes systemic conditions that have nothing to do with the eye on the surface, diabetes, high blood pressure, heart disease, asthma, or autoimmune disease, along with any current medications and known allergies. Glaucoma management decisions are frequently shaped by what is happening in the rest of your body, so none of this is skipped.
Three vision measurements, not one
Your vision is then checked through a formal refraction, and three separate numbers are recorded:
- UCVA, your uncorrected visual acuity, what you see with no glasses at all
- PGP, your vision with the glasses you are currently wearing and prescribed
- BCVA, your best corrected visual acuity, what you could see with the ideal glasses prescription
Comparing these three numbers tells me whether a vision problem is about your eyewear, your ocular surface, or your optic nerve, before I have even examined you. A non contact tonometry pressure check is occasionally done at this stage as a screening step. I insist on Goldmann Applanation Tonometry for all of my glaucoma patients.
Step 2: I Review Your History and Examine the Front of the Eye
When you come in to see me, I read through everything the optometrist has documented at a glance. If anything looks incomplete, inconsistent, or worth a second look, I will ask more specific questions to understand it properly before moving forward.
There is also, always, a few minutes of ordinary conversation. A glaucoma consult is a long term relationship, not a transaction. It starts with treating you like a person before a set of test results. And you will be shocked at the details I remember. Your family, your last vacation, your dog 🙂 sometimes, even your favourite chutney!
I then examine the front of your eye in detail. The conjunctiva and ocular surface, the meibomian glands, the eyelid and bulbar conjunctiva, the anterior chamber, and the lens, looking specifically for cataract, a shallow anterior chamber, or any cells in the anterior chamber (inflammation).
Step 3: A Deliberate Order of Testing, Not a Random Checklist
The sequence in which glaucoma tests are performed matters, and I follow a fixed order rather than doing whichever test is most convenient.
Angle assessment first, with imaging informing the decision
I assess the optic nerve with a 90 dioptre lens. Every glaucoma patient gets a gonioscopy. When you need a repeat gonioscopy is decided after that. I perform it only after the visual field test, the OCT, and fundus photography are done, when those are part of that visit. Imaging the nerve and the visual field before manipulating the angle gives me a cleaner functional and structural baseline to work from.
Central corneal thickness, then pressure, then gonioscopy
Before gonioscopy, I measure central corneal thickness (CCT), the test also called pachymetry. Corneal thickness directly affects how your raw eye pressure reading should be interpreted. But it is always done before your tonometry. Because touching your corneas to measure your IOP before the CCT may alter it slightly. Gonioscopy then follows. This examines your drainage angle under magnification. This determines whether you have an open angle or a narrow angle profile.
Why I do the pressure check myself
Goldmann applanation tonometry (GAT), the test that measures your intraocular pressure, is the one test I do not delegate. In my clinic, I personally perform this for every glaucoma patient before treatment starts. Again at the first follow up, and at every annual review. My optometrists are trained to do it and do perform it in my absence. Doing it myself gives me a direct feel for what is happening in your eye that a number on a chart cannot fully convey.
I also insist on doing my gonioscopy myself, always with the lights switched off, so be prepared for a few minutes in a dark room. I keep talking to you, so its never scary.
How is Applanation Tonometry Done?
For the GAT, one of my team members will put some numbing eyedrops and ask you not to touch your eye. I then put a dye which stains your tears yellow. And then I check your eye pressures under blue light on the slit lamp, with a prism that comes close to the eye.
It takes less than a minute if you don’t blink and keep looking straight ahead, and a few extra seconds if you fidget. It’s painless, and quick, and we finish with a drop of antibiotic in the eye.
Step 4: Dilation, When It Is Needed
If your assessment requires dilating your pupils, you will be told this in advance, because dilation takes about forty five minutes to take full effect and changes how you experience the rest of your day.
- We ask you to bring dark glasses, a scarf, or an umbrella, since dilated eyes are far more light sensitive, particularly in Gurugram’s daytime heat
- We advise you not to drive yourself home after a dilated examination
Step 5: Establishing a True Baseline, Not a Single Snapshot
Glaucoma decisions should never rest on one reading taken on one day. Two specific habits in my clinic exist to correct for that.
Repeating your first visual field
There is a genuine learning curve to taking a visual field test well. The first attempt is frequently unreliable simply because the patient has not yet learned the rhythm of the test. I routinely discard the first visual field and ask patients to return the next morning. We do not charge for that repeat test. The inaccuracy is a known limitation of the test itself, and is not a reason to bill twice.
Three pressure readings, not one
For a true baseline, I usually take three intraocular pressure readings at different times of day. Rather than relying on a single number, since pressure naturally fluctuates through the day. One of these three readings may be taken by an optometrist, if it’s after my working hours. We usually work from the average of all three.
The water drinking test
A formal diurnal variation test, in which pressure is measured every few hours through the day, is not practical for every patient. We often use the water drinking test as a more practical stand in. This is typically done before starting treatment, again about one to two months after treatment begins. We may repeat it if your eye appears to be progressing despite your pressure meeting its target.
Step 6: Setting Your Personalised Target Pressure
There is no single universal normal pressure number in modern glaucoma care. Your corneal thickness, the structure of your drainage angle, and your Visual field and OCT baseline are combined to calculate a target pressure zone. This is specific to your eye, designed to halt progression for you.
Step 7: The Most Important Section of Glaucoma Consultation: Eye Drop Training
A prescription on its own does not protect your vision if the drops never go in correctly or are forgotten. So every consult ends with practical training, not just instructions.
- I personally show you how to instil your eye drops correctly, since technique affects how much medication actually reaches the eye
- I ask you to set a phone alarm for every dose. Because relying on memory alone is the most common reason treatment fails
- If you are on more than one medication, I recommend keeping two small boxes. One empty and one full of your drop bottles. After each dose, you move that bottle from the full box to the empty one. So a glance at the boxes tells you whether you have already taken that round of drops. And which ones remain.
- When you leave, my coordinator helps you set your next appointment, before you leave the clinic. You will also receive a Whatsapp message with links to important information and details of phone numbers to book appointments. You will also get my direct phone number for any clinical queries, or emergencies.
When To See Me Before Your Booked Glaucoma Consultation
- Sudden eye pain, redness, or blurred vision, which can signal an acute angle closure attack
- Any one sided change in vision or eye appearance
- Headache or nausea accompanying eye pain
- A noticeable change in your visual field between scheduled visits
- New side effects after starting or changing a glaucoma medication
- Missed doses for several consecutive days, which should be flagged at your next visit rather than left unmentioned
This page is a part of the Glaucoma Hub. you may want to read about Glaucoma Progression, and Risk Stratification in Glaucoma. Other articles of interest could be Advanced Glaucoma Care in Gurgaon, What Good Glaucoma Care Actually Optimises For, What Happens If Glaucoma Is Left Untreated?, More Glaucoma Eye Drops is Not Better Glaucoma Care, 5 Mistakes Patients Make in Glaucoma Care and Do You Really Need Treatment for Glaucoma?
Frequently Asked Questions
Why does the optometrist see me before the doctor does?
The optometrist’s workup, history, refraction, and the three part vision check, ensures your file is complete and your baseline vision is documented accurately before I begin my own examination. This makes the time I spend with you more focused on interpretation and decision making rather than data collection.
Why do you measure my eye pressure yourself instead of leaving it to staff?
Goldmann applanation tonometry is the gold standard pressure test, and for every glaucoma patient I treat, I perform it myself before starting treatment, at the first follow up, and at every annual review. It gives me a direct sense of your eye’s behaviour that I do not want to lose by always delegating it.
Why do you discard my first visual field test and ask me to repeat it?
Most patients have not yet learned the rhythm of the visual field test on their first attempt. This makes that first result unreliable. We ask you to return the next morning for a repeat test. We do not charge for it, since the inaccuracy belongs to the learning curve of the test, not to you.
Why is gonioscopy done after OCT and visual field testing, not before?
When OCT, visual field testing, and fundus photography are part of your visit, I prefer to have that structural and functional picture in hand before manipulating the angle during gonioscopy. The order is chosen to give the cleanest possible baseline. Also, sometimes I use a viscoelastic gel for gonioscopy. In that case, your vision is fuzzy for about ten minutes after, and I don’t want your time wasted.
What is the water drinking test and why would I need one?
It is a practical way of checking how your eye pressure responds to a physiological stress. This is used in place of round the clock diurnal variation testing, which is not feasible for every patient. I typically use it before starting treatment. I may repeat it again a month or two into treatment. And again later if your eye appears to be progressing even though your pressure looks controlled.
Why do you spend time teaching me to put in my own eye drops?
Technique directly affects how much medication reaches your eye. A missed or mistimed dose is the most common reason glaucoma treatment underperforms. Pairing a phone alarm with the two box system is simple. It gives you a simple, visual way to know whether today’s dose has already gone in. Research says it is the most important intervention in preventing glaucoma blindness.
Key Takeaways
- Your consult begins with the optometrist. They document history and perform three vision measurements, UCVA, PGP, and BCVA, before I examine you
- Testing follows a fixed order: imaging and visual field first when needed, then corneal thickness, then gonioscopy, then pressure measurement
- I personally measure your eye pressure for every glaucoma patient at key visits, rather than delegating it
- Your first visual field is usually repeated free of charge, because of a genuine learning curve with the test
- Baseline pressure is built from three readings at different times of day, sometimes supplemented by a water drinking test
- Your target pressure is personalised to your eye’s anatomy, not based on one generic normal number
- No consult ends without hands on training in how to use your drops. And how to track whether you have taken them
Book a Consultation
If you have been told you have glaucoma, or are due for a routine check because of family history or elevated pressure, this is the process you can expect to walk through.
[Book an Appointment →www.drshibalbhartiya.com | +91 88826 38735]
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
1500+ Five Star Patient Reviews Google Business Profile
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation
Read her research on PubMed | Google Scholar | ResearchGate | ORCID
Upload your reports for a structured review.| www.drshibalbhartiya.com | +91 88826 38735
Leave a review on Google