Glaucoma progression despite apparently controlled intraocular pressure is one of the most disorienting experiences a patient can face. It is also one of the most common reasons patients seek a glaucoma second opinion. The reason is almost always the same: daytime clinic readings capture one moment. They do not capture what happens at night, explains Dr Shibal Bhartiya.
Not all glaucoma medications lower pressure around the clock. Brimonidine and timolol both show significantly reduced activity after midnight. A patient whose pressure is controlled at 11 am may have entirely uncontrolled pressure at 3 am — and no standard clinic visit will reveal this.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
My Glaucoma Is Progressing But My Pressure Is Always Normal. What Is Going On?
He was in his early sixties — careful, informed, and deeply confused.
He came to me for a second opinion after five to six years under glaucoma care. His file was meticulous. His lifestyle was exemplary — non-smoker, controlled blood pressure, controlled blood sugars. He was on two medications: timolol and brimonidine. His baseline IOP had been 26 to 27 mmHg. On treatment, it now sat at 13 to 14 mmHg at every clinic visit for years.
By every standard measure, he was a success story. But his glaucoma was still progressing.
He was not angry. He was bewildered. I have done everything right, he told me. Why is this still happening?
That question deserved a better answer than he had been given. The answer was in the hours nobody had measured.
The question nobody had asked
I looked at his records and asked him one thing: had anyone ever done a diurnal variation for him? A 24-hour IOP measurement, mapped across day and night? Or a Water Drinking Test?
He said no.
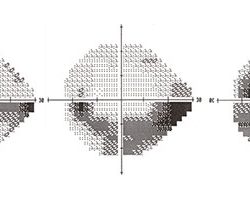
We enrolled him in a study using the Triggerfish sensor — a contact lens device that records continuous IOP fluctuation over 24 hours. The device does not measure absolute pressure values, but it maps the pattern of fluctuation with precision.
The night-time readings were almost double the daytime values.
Most clinic visits measure pressure once, mid-morning, when he was up and about. That is the reading least likely to catch a nocturnal spike. His reassuring numbers, always 13, always 14, had been capturing only half the story. The other half was unfolding while he slept, while no one was measuring, while his optic nerve absorbed damage that nobody anticipated.
Why his medications were failing him at night
The reason was pharmacological, and it is something worth stating clearly: brimonidine and timolol do not work at night. Their pressure-lowering effect drops sharply in the late hours. His reassuring clinic readings — always 13, always 14 — had been capturing only half the story. The other half was invisible, unfolding while he slept, while no one was measuring, while his optic nerve absorbed damage that nobody anticipated.
This is not a failure of the medications. It is a failure of the measurement system — and of the assumption that a daytime number tells the whole story.
What Doctors Often Miss
Brimonidine and timolol do not work at night. This is pharmacology, not failure — their pressure-lowering effect drops sharply in the late hours. It is a well-documented limitation that is not always communicated to patients or factored into treatment decisions.
The result is that a patient can have genuinely excellent daytime control and entirely uncontrolled nocturnal pressure simultaneously. Standard clinic visits — timed to office hours — will never detect this.
The other missed step is the diurnal variation test itself. It is one of the most underused and highest-yield investigations in glaucoma management. It is rarely ordered unless a specialist specifically suspects nocturnal IOP spikes. If your glaucoma is progressing despite apparently good readings, this investigation is worth asking for by name — and a glaucoma second opinion is always reasonable in this situation.
Why Prostaglandins Are First-Line for a Reason
We switched him to bimatoprost 0.01% — a prostaglandin analogue. Prostaglandins are the only class of glaucoma medication proven to work continuously across 24 hours. They do not lose activity at night.
That was in 2012 to 2013. He has been stable for over six years.
One molecule change. One question that had never been asked. Six years of stability that five years of treatment had never delivered.
Symptoms, Pressure Patterns, and When to Investigate
| Finding | Likely Cause | When to Investigate Further |
|---|---|---|
| Glaucoma progressing despite good clinic IOP | Nocturnal IOP spike not captured by daytime readings | Request 24-hour diurnal variation assessment |
| On timolol or brimonidine, still progressing | Night-time loss of drug efficacy | Ask whether a prostaglandin has been considered |
| Visual field deterioration at routine review | Ongoing IOP fluctuation between clinic visits | IOP fluctuation may be as damaging as sustained elevation |
| Good compliance, good lifestyle, still progressing | Medication class mismatch for 24-hour coverage | Second opinion from glaucoma specialist |
| Pressure controlled but OCT showing RNFL thinning | Structural damage continuing despite IOP numbers | Full diurnal assessment and treatment review |
What This Means for You
If your glaucoma is progressing despite readings that look controlled, the readings may be incomplete — not the whole story, only the morning chapter.
The questions worth asking at your next visit: Has my pressure ever been measured at night? Has anyone checked whether my medications work across 24 hours? Has a prostaglandin analogue been considered as my primary medication?
You are not doing anything wrong. The measurement system may simply be missing the hours that matter most.
If your glaucoma is progressing despite treatment, or if you have never had a 24-hour IOP assessment, a specialist review may give you answers years of routine care have not.
Book a consultation or second opinion with Dr Shibal Bhartiya in Gurgaon.
+91 88826 38735 | www.drshibalbhartiya.com
FAQs
My glaucoma is progressing but my eye pressure is always normal at the clinic. How is that possible?
Clinic readings capture pressure at one moment, usually mid-morning. Eye pressure fluctuates across 24 hours. Certain medications — including timolol and brimonidine — lose effectiveness at night. If pressure spikes at 2 am, no daytime clinic visit will catch it. That spike is still damaging your optic nerve, invisibly, visit after visit.
What is a diurnal variation test and do I need one?
A diurnal variation maps your eye pressure across the full day and night. It is recommended when glaucoma is progressing despite apparently controlled pressure, when you are on medications that may not provide round-the-clock coverage, or when your specialist suspects night-time IOP spikes. It is one of the most underused and highest-yield tests in glaucoma management.
Why are prostaglandin eye drops the first choice for glaucoma?
Prostaglandins are the only class of glaucoma medication that works continuously across 24 hours. Other drugs — including timolol and brimonidine — show significantly reduced activity at night. For long-term pressure control, the night-time hours matter as much as the daytime ones. This is why prostaglandin analogues are recommended as first-line therapy in international glaucoma guidelines.
Can glaucoma progress even when I am doing everything right?
Yes, and it is more common than patients realise. Controlled daytime pressure, healthy lifestyle, medication compliance — none of these guarantee protection if night-time IOP is unaddressed. Progression despite apparent control is a signal to investigate further, not to doubt yourself. A glaucoma second opinion is always reasonable in this situation.
Should I ask for a 24-hour IOP test if my glaucoma is progressing?
Yes. If your visual fields are declining despite good clinic readings, a diurnal variation assessment is a reasonable and important next step. Ask your glaucoma specialist specifically about this. It is a question worth asking at your next visit.
This page is part of the Advanced Glaucoma Care hub. Read about the full spectrum of glaucoma diagnosis and treatment. Please also read about Diurnal Variation of IOP, Target IOP and Glaucoma Eye Drops.
You may want to watch this podcast I did several years ago, for Health Talks.
Note: Contact Lens Monitor for Continuous IOP Monitoring
Triggerfish® contact lens sensor is a specialised diagnostic contact lens used in glaucoma care to monitor intraocular pressure (IOP)–related changes over 24 hours. Unlike routine pressure measurements taken during clinic hours, the Triggerfish lens (Sensimed Triggerfish) helps detect pressure fluctuations that may occur at night or outside OPD visits, which can sometimes explain progression despite apparently controlled readings. It does not measure pressure directly in mmHg but records circumferential corneal changes related to IOP patterns, helping glaucoma specialists better understand individual risk profiles and treatment needs in selected patients.
Dr Shibal Bhartiya was the first doctor in India to use the Triggerfish® contact lens sensor for Continuous IOP Monitoring in clinical practice. Her initial experiences on Intraocular pressure (IOP) related pattern in patients with primary angle closure (PAC) and primary angle closure glaucoma (PACG) before and after laser peripheral iridotomy (LPI) was presented at ARVO, in Orlando Florida in 2014
IOP Fluctuation and Angle Closure Glaucoma
IOP fluctuation is a particular concern in angle closure disease, where pressure spikes can be steep and are frequently missed by routine daytime readings. Dr Bhartiya’s published research has examined this directly. A 2015 study in the Journal of Current Glaucoma Practice, Diurnal Intraocular Pressure Fluctuation in Eyes with Angle-Closure (Bhartiya S, Ichhpujani P; PMID: 26997828), investigated IOP fluctuation across the day in 77 newly diagnosed angle closure patients and documented the range and pattern of diurnal variation in this group.
A 2019 review in the Romanian Journal of Ophthalmology, Diurnal Variation of IOP in Angle Closure Disease: Are We Doing Enough? (Bhartiya S et al.; PMID: 31687621), went further — finding that many clinical decisions in angle closure glaucoma management are based on only one or two IOP measurements, and arguing that this is insufficient given the established circadian rhythm of IOP and its direct correlation with glaucoma progression. Taken together, these papers make the case that angle closure patients may be among the most undertreated precisely because their worst pressure moments are the least observed.
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (PubMed-indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks, span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
1,500+ Five Star Patient Reviews — Google Business Profile
Read her research on PubMed | Google Scholar | ResearchGate | ORCID
Upload your reports for a structured review. | www.drshibalbhartiya.com | +91 88826 38735
Leave a review on Google