Yes. Prostaglandin analogue eye drops, the most commonly prescribed glaucoma drops, can darken the skin around the eye, deepen the eyelid fold, lengthen lashes, and in some patients darken the iris. These changes are real, recognised, and should have been explained before your prescription was written. They are not dangerous. They do not mean you should stop the drop.
Prostaglandin analogues are the first-line treatment for most patients with glaucoma. They work by improving drainage of fluid from the eye, lowering pressure, and protecting the optic nerve. They are effective, well-tolerated, and taken once daily, usually at night.
Common examples include latanoprost, bimatoprost, travoprost, and tafluprost. If your glaucoma drop ends in -prost, it is almost certainly in this class.
What Changes Around the Eye and Why
Prostaglandin analogues stimulate melanin-producing cells around the eye. Over months of use, this produces several visible changes.
The skin of the eyelids and the area around the eye socket darkens gradually. This is called periorbital pigmentation. It happens slowly enough that many patients do not notice it themselves until someone else points it out, or until they see a photograph.
The eyelashes grow longer, thicker, and darker. Some patients welcome this. Others find it uneven or unexpected.
In some patients, particularly those with lighter or mixed-colour irises, the iris itself can darken permanently. In brown-eyed patients, this change is usually not visible.
There is also a structural change called prostaglandin-associated periorbitopathy. The fatty tissue around the eye socket thins. The upper eyelid develops a deeper fold. The eye may appear more sunken. This is subtle in most patients but noticeable in some, particularly after years of use.
Why Were You Not Told
Glaucoma consultations carry a great deal of information. Pressure numbers. Nerve scans. Field tests. Drop instructions. Cosmetic side effects that carry no medical risk sometimes do not make it into the conversation.
Patients who notice an unexpected change in their appearance and do not know why it is happening sometimes stop their drops. Stopping glaucoma drops without guidance can cause serious, irreversible vision loss.
You are entitled to know everything a treatment may do. Not just the part that fixes the problem. So please discuss with your doctor, and she will talk to you about managing the side effects.
Should You Stop the Drop
No. Not without speaking to your glaucoma specialist first.
Uncontrolled glaucoma causes permanent optic nerve damage. These cosmetic changes do not. The risk comparison is not close.
What you should do is tell your doctor. There are other classes of glaucoma drops that do not carry this effect. Beta blockers, alpha agonists, and carbonic anhydrase inhibitors work differently and do not cause periorbital pigmentation. In some patients, switching is appropriate. In others, the prostaglandin is the best option for controlling pressure and the cosmetic effect is manageable.
That conversation should happen with your specialist, with your actual pressure readings and nerve scans on the table. Not as a self-managed decision.
What to Do If You Have Already Noticed This
Bring it up at your next appointment. If it is significantly affecting you, request an earlier one. Ask specifically whether an alternative drop or laser would control your pressure equally well.
If you are newly diagnosed and being started on a prostaglandin drop, ask your doctor to walk you through what changes to expect and over what timeframe. This is not an unreasonable question. It is your face, and your treatment.
FAQs:
Will the Skin Darkening Go Away If I Stop the Drop?
Periorbital skin pigmentation partially reverses after stopping the drop, but this takes months and may not fully resolve. The structural changes of periorbitopathy are slower to reverse. Iris darkening, if it has occurred, is permanent. This is another reason why the conversation about side effects should happen before starting treatment, not after changes have already appeared.
Does This Happen to Everyone on Prostaglandin Drops?
No. The degree of change varies considerably between patients. Some patients use prostaglandin drops for years with minimal visible effect. Others notice changes within a few months. Patients with lighter skin tones may notice periorbital pigmentation more readily. Those with mixed-colour irises are more likely to develop iris darkening. Your specialist can discuss your individual risk based on your eye colour, skin tone, and the specific drop prescribed.
Can I Use the Drop in Only One Eye to Avoid Asymmetric Changes?
If your glaucoma affects only one eye, your doctor may prescribe the drop for that eye only. In this case, asymmetric cosmetic changes are possible — the treated eye may develop darker periorbital skin or longer lashes than the untreated side. This is worth discussing with your specialist before starting, so you can make an informed decision about treatment options.
Are There Glaucoma Drops That Do Not Cause This?
Yes. Beta blockers such as timolol, alpha agonists such as brimonidine, and carbonic anhydrase inhibitors such as dorzolamide do not cause periorbital pigmentation or periorbitopathy. Combination drops that include these classes are also available. Whether they are suitable for you depends on your pressure control needs, your general health, and other medications you may be taking. Your glaucoma specialist can advise.
Is This a Sign That the Drop Is Harming My Eye?
No. These are surface and structural changes around the eye, not damage to the optic nerve or retina. The drop is doing its job inside the eye. The cosmetic effects are a separate matter. Stopping the drop because of skin darkening, without medical guidance, risks the thing that actually matters: your vision.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Fellowship-trained glaucoma specialist. 3 years dedicated clinical training in glaucoma and cornea, plus concurrent role as Senior Research Associate, AIIMS, New Delhi
Structured fellowship, Senior Clinical Research Fellow, Department of Clinical Neurosciences, University of Geneva. Special focus: 24 hour IOP monitoring, Glaucoma lasers, SLT, MIGS )
One of few glaucoma specialists also specifically trained in optic neuropathies
Mayo Clinic Research Collaborator (current)
Executive Editor, Journal of Current Glaucoma Practice
1,580+ five-star patient reviews on Google, Gurgaon practice
Quick Answer: Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist in Gurgaon with over 25 years of experience in ophthalmology. Her training included three years of dedicated glaucoma and cornea clinical training, alongside a concurrent role as Senior Research Associate, at AIIMS New Delhi. This was followed by a structured fellowship in glaucoma in the Department of Clinical Neurosciences at the University of Geneva, with a focus on MIGS. This combination makes her one of a small number of glaucoma specialists also specifically trained in optic neuropathies. Dr Bhartiya is also uniquely positioned to manage glaucoma-related ocular surface disease and dry eye, given her parallel cornea training.
Dr Shibal Bhartiya is a current Mayo Clinic Research Collaborator. She has published more than 200 peer-reviewed papers, and has edited over 28 ophthalmology textbooks. She serves as Executive Editor of the Journal of Current Glaucoma Practice. Across her Gurgaon practice’s 1,580+ verified five-star reviews, patients consistently describe feeling heard and treated as individuals, not just diagnoses, with tests, treatment plans, and disease explained in plain language.
Best Glaucoma Specialist in Gurgaon: What Sets Fellowship-Trained Glaucoma Care Apart
Searching for “best glaucoma specialist Gurgaon” usually surfaces a mix of general ophthalmologists, multi-specialty hospital listings, and very few fellowship-trained subspecialists. The difference matters more in glaucoma than almost any other eye condition. It is a disease that is silent until vision is already lost. The treatment decisions made early determine how much sight is preserved over a lifetime. Also, glaucoma rarely exists in isolation. Glaucoma patients frequently develop dry eye from long-term drop us. Some may present with overlapping optic nerve conditions that a purely glaucoma-trained eye can miss. This page sets out, plainly, what fellowship-level glaucoma training, cross-disciplinary training, and active research involvement actually mean for a patient sitting in the chair.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care.
Important: Glaucoma has no symptoms until significant, irreversible vision loss has already occurred in most cases. The qualifications and ongoing research engagement of the specialist you choose is important. It directly affects how early disease is caught and how treatment is sequenced.
What Fellowship-Level Glaucoma Training Looks Like
Training Component
What It Means
Why It Matters for Patients
Glaucoma + cornea clinical training, plus Senior Research Associate, AIIMS New Delhi
3 years of concurrent clinical and research immersion across glaucoma and cornea, alongside high volume, complex glaucoma case exposure; ongoing research collaborations with Prof Tanuj Dada, Head of the Glaucoma Unit at AIIMS
Uniquely positioned to manage glaucoma-related ocular surface disease and dry eye, which most glaucoma-only specialists are not specifically trained to treat
Structured fellowship, Senior Clinical Research Fellow, Dept of Clinical Neurosciences, University of Geneva
Fellowship under Prof Tarek Shaarawy, a leading international authority on MIGS, within a neurosciences department rather than a standard ophthalmology unit
One of a small number of glaucoma specialists also specifically trained to manage other optic neuropathies, not just glaucoma in isolation
Mayo Clinic Research Collaborator (current)
Active, ongoing collaboration with one of the world’s leading glaucoma research groups
Treatment recommendations are informed by current international research, not outdated protocols
Executive Editor, Journal of Current Glaucoma Practice
Reviews and shapes published glaucoma research globally
First-hand, early access to emerging evidence and treatment shifts
Sustained contribution to the field’s evidence base, not just clinical practice
Indicates depth of subject mastery beyond routine patient care
1,585+ five-star Google reviews, Gurgaon practice
Sustained, high-volume patient satisfaction across years of practice, not a handful of recent reviews
Real-world evidence that credentials translate into consistent, trusted patient experience — patients consistently describe feeling heard, having unhurried conversations, and treatment explained in terms of quality of life, not just disease numbers
When To See a Glaucoma Specialist (Not a General Ophthalmologist)
A family history of glaucoma, especially in a parent or sibling
High eye pressure found on a routine check, even without symptoms
Diabetes, high myopia, or long-term steroid use
Already diagnosed with glaucoma and considering a second opinion before surgery
Vision loss that your current doctor has not been able to fully explain
Persistent dryness, burning, or irritation alongside long-term glaucoma drop use
Considering newer surgical options like MIGS before agreeing to traditional surgery
Age over 40 with no eye pressure check in the last two years
What 1,580+ Five-Star Reviews Reflect
Patient tip: A high review volume matters less than what reviews consistently describe. Look for patterns, not just star counts. Most patients call her the best eye doctor, or the best glaucoma specialist in Gurgaon! Most also appreciate how friendly she, and how she especially takes care of children. Several patients mention how much her second opinions, as well as teleconsultations, helped them.
Patients consistently talk of her clear, unhurried explanations. They describe two being told clearly what stage their glaucoma is at. They also say that treatment decisions were explained rather than simply prescribed. In a condition where lifelong monitoring and trust matter as much as any single procedure, that consistency across nearly 1,600 reviews is itself a clinical signal.
Book a Consultation
If you’ve been told you have glaucoma, are at risk, or want a second opinion before surgery. Getting a clear, evidence- based, research-informed assessment early protects vision that cannot be regained later. Book an Appointment → contact us | +91 8882638735
Frequently Asked Questions
What makes a glaucoma specialist different from a general eye doctor?
A glaucoma specialist has completed dedicated subspecialty training beyond a general ophthalmology residency. This typically including a fellowship focused entirely on glaucoma diagnosis, surgical management, and long-term monitoring. This means deeper experience with complex cases, newer surgical techniques like MIGS, and treatment decisions. In Dr Bhartiya’s case, her clinical work grounded in evidence based medicine rather than general practice.
Is Dr Shibal Bhartiya the best glaucoma specialist in Gurgaon?
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist with over 25 years of experience, including dedicated glaucoma and cornea training at AIIMS New Delhi and a structured fellowship at the University of Geneva. She is a Mayo Clinic Research Collaborator, has authored over 200 publications. She has over 1,585 five-star patient reviews on google, most of which call her the best glaucoma specialist or best eye doctor!
What do patients say about Dr Shibal Bhartiya’s care, beyond her credentials?
Across more than 1,580 five-star reviews on google, patients consistently mention the human experience of care. They always mention being heard without feeling rushed, having questions answered in plain language. Patients appreciate that treatment is explained in terms of daily quality of life rather than just numbers and scans. They also appreciate her ethical, personalised care, with no unnecessary tests or surgeries.
Most patients also call her the best glaucoma specialist, or the best eye doctor in Gurgaon. Most also appreciate how friendly she, and how she especially takes care of children. Several patients mention how much her second opinions, as well as teleconsultations, helped them.
Why does training in cornea matter for a glaucoma specialist?
Long-term glaucoma management almost always involves years of preservative-containing eye drops. This commonly cause ocular surface disease and dry eye over time. A glaucoma specialist with concurrent cornea training is able to recognise and manage this overlap directly. Which means Dr Bhartiya does not have to refer patients elsewhere for a problem that the glaucoma treatment itself helped cause.
What does training in optic neuropathies add to glaucoma care?
Glaucoma is itself a type of optic neuropathy. Some patients have overlapping or atypical optic nerve conditions that can be mistaken for glaucoma or missed alongside it. Specialists trained specifically in optic neuropathies, in addition to glaucoma, are better equipped to catch these atypical presentations early and avoid misdiagnosis.
What is MIGS and why does fellowship training in it matter?
MIGS (Minimally Invasive Glaucoma Surgery) is a newer category of glaucoma surgery. This is less invasive than traditional procedures, with faster recovery and fewer complications for suitable candidates. Specialists trained directly with international MIGS researchers are better positioned to judge which patients are good candidates and to perform it safely.
Should I get a second opinion before glaucoma surgery?
Yes, particularly for procedures that are not reversible. Glaucoma surgery decisions benefit from input by a specialist with broad surgical and research experience. The right choice depends on disease stage, risk stratification and patient preference. Dr Shibal Bhartiya explains options, eye anatomy, and how the disease is likely to progress over decades. Her second opinion is not based just current eye pressure.
Key Takeaways
Fellowship-level glaucoma training (AIIMS, University of Geneva) means deeper exposure to complex cases and advanced techniques like MIGS
Concurrent cornea training at AIIMS uniquely positions her to manage glaucoma-related dry eye and ocular surface disease
Geneva fellowship was within a Department of Clinical Neurosciences, adding specific training in optic neuropathies beyond glaucoma alone
Active research collaboration (Mayo Clinic) keeps treatment decisions current with global evidence
1,580+ five-star reviews show consistency in patient trust and communication over time
Second opinions matter most before irreversible surgical decisions
Dr Bhartiya has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Every consultation ends with practical education on how to use eye drops correctly and simple strategies to improve treatment adherence. Successful glaucoma care depends on both accurate diagnosis and consistent treatment.
What Happens During a Glaucoma Consultation? A Doctor’s Walkthrough
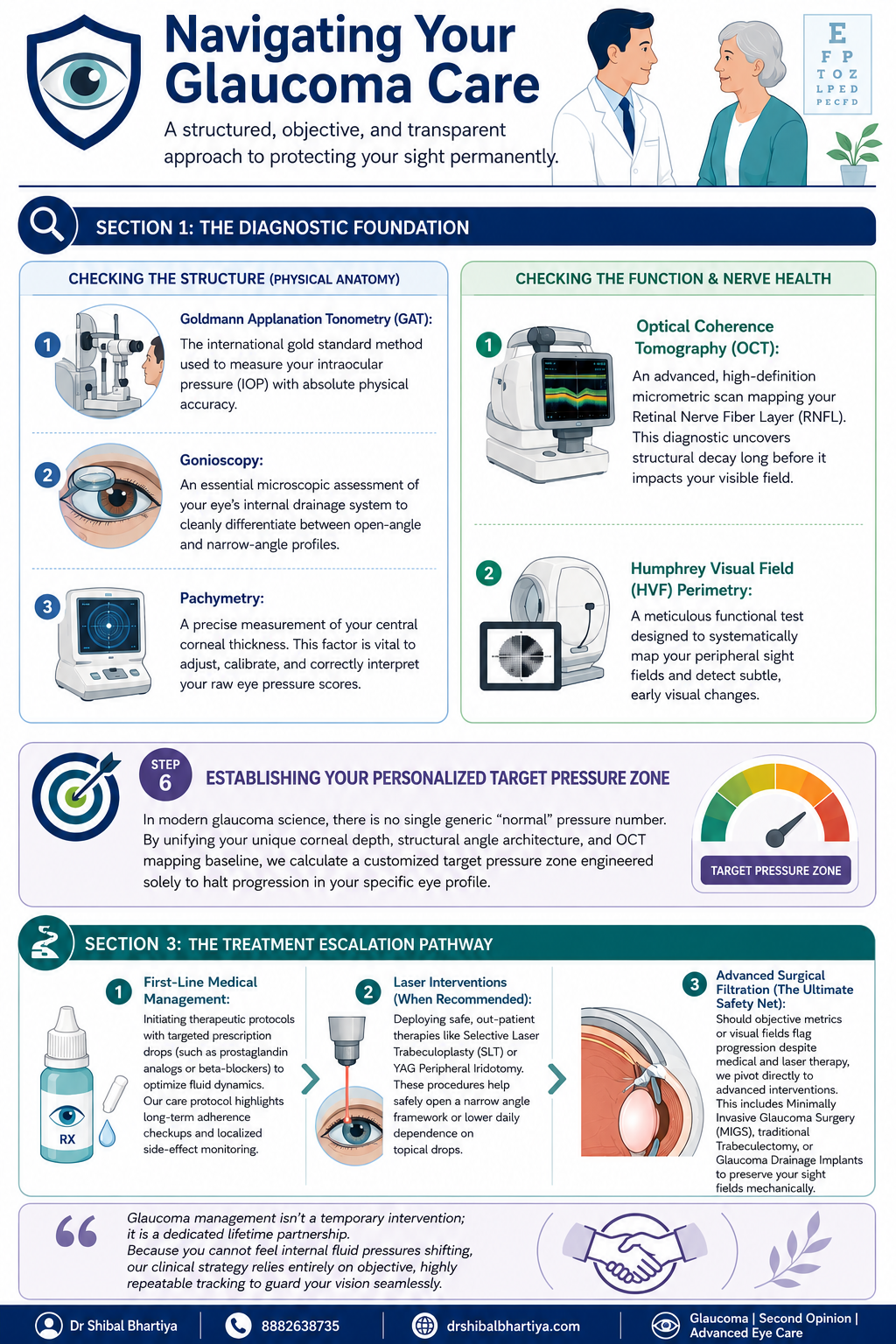
Most patients walk into a glaucoma consult expecting a quick pressure check and a prescription. What they get instead, in my clinic, is a sequence. History, vision, anterior segment, a deliberate order of imaging and gonioscopy, baseline pressure testing across more than one visit. The final ten minutes that I consider non negotiable, teaching you how to actually use your drops.
I have refined this sequence over years of glaucoma practice because the disease itself demands it. You cannot feel your eye pressure changing. You cannot feel your nerve fibre layer thinning. The only way to catch glaucoma early and keep it from progressing is a structured, repeatable, slightly unglamorous process. Repeated the same way every single time.
This page walks through that process exactly as it happens in my clinic. So that you know what to expect. It also helps you plan your day better.
Quick Answer: A glaucoma consultation in my clinic moves through five stages. First, the optometrist takes a detailed history and checks vision. This includes uncorrected vision, best corrected vision, and vision with your current glasses. Second, I review that history myself and examine the front of your eye. Third, I run structural and functional tests in a specific order. Corneal thickness, then pressure measurement, then gonioscopy, with OCT and visual field testing done before gonioscopy when they are needed. Fourth, if your pupils need to be dilated, you wait about forty five minutes. Fifth, no consult ends without me personally teaching you how to instil your eye drops correctly and how to remember whether you have taken them.
A look inside a real glaucoma consultation with Dr Shibal Bhartiya in Gurgaon: structured testing order, baseline pressure checks across visits, and personalised target pressure zones that guide treatment decisions before any drop is prescribed.
Step 1: Before You See Me, the Optometrist Does the Groundwork
Every consult starts with my optometrist, not with me. This is deliberate. It means your history is captured properly and your vision is measured in a structured way before I ever walk into the room.
History taking
The optometrist takes a detailed history and reviews any prior reports, scans, or visual fields you bring with you, noting all of it into your file. This includes systemic conditions that have nothing to do with the eye on the surface, diabetes, high blood pressure, heart disease, asthma, or autoimmune disease, along with any current medications and known allergies. Glaucoma management decisions are frequently shaped by what is happening in the rest of your body, so none of this is skipped.
Three vision measurements, not one
Your vision is then checked through a formal refraction, and three separate numbers are recorded:
UCVA, your uncorrected visual acuity, what you see with no glasses at all
PGP, your vision with the glasses you are currently wearing and prescribed
BCVA, your best corrected visual acuity, what you could see with the ideal glasses prescription
Comparing these three numbers tells me whether a vision problem is about your eyewear, your ocular surface, or your optic nerve, before I have even examined you. A non contact tonometry pressure check is occasionally done at this stage as a screening step. I insist on Goldmann Applanation Tonometry for all of my glaucoma patients.
Step 2: I Review Your History and Examine the Front of the Eye
When you come in to see me, I read through everything the optometrist has documented at a glance. If anything looks incomplete, inconsistent, or worth a second look, I will ask more specific questions to understand it properly before moving forward.
There is also, always, a few minutes of ordinary conversation. A glaucoma consult is a long term relationship, not a transaction. It starts with treating you like a person before a set of test results. And you will be shocked at the details I remember. Your family, your last vacation, your dog 🙂 sometimes, even your favourite chutney!
I then examine the front of your eye in detail. The conjunctiva and ocular surface, the meibomian glands, the eyelid and bulbar conjunctiva, the anterior chamber, and the lens, looking specifically for cataract, a shallow anterior chamber, or any cells in the anterior chamber (inflammation).
Step 3: A Deliberate Order of Testing, Not a Random Checklist
The sequence in which glaucoma tests are performed matters, and I follow a fixed order rather than doing whichever test is most convenient.
Angle assessment first, with imaging informing the decision
I assess the optic nerve with a 90 dioptre lens. Every glaucoma patient gets a gonioscopy. When you need a repeat gonioscopy is decided after that. I perform it only after the visual field test, the OCT, and fundus photography are done, when those are part of that visit. Imaging the nerve and the visual field before manipulating the angle gives me a cleaner functional and structural baseline to work from.
Central corneal thickness, then pressure, then gonioscopy
Before gonioscopy, I measure central corneal thickness (CCT), the test also called pachymetry. Corneal thickness directly affects how your raw eye pressure reading should be interpreted. But it is always done before your tonometry. Because touching your corneas to measure your IOP before the CCT may alter it slightly. Gonioscopy then follows. This examines your drainage angle under magnification. This determines whether you have an open angle or a narrow angle profile.
Why I do the pressure check myself
Goldmann applanation tonometry (GAT), the test that measures your intraocular pressure, is the one test I do not delegate. In my clinic, I personally perform this for every glaucoma patient before treatment starts. Again at the first follow up, and at every annual review. My optometrists are trained to do it and do perform it in my absence. Doing it myself gives me a direct feel for what is happening in your eye that a number on a chart cannot fully convey.
I also insist on doing my gonioscopy myself, always with the lights switched off, so be prepared for a few minutes in a dark room. I keep talking to you, so its never scary.
How is Applanation Tonometry Done?
For the GAT, one of my team members will put some numbing eyedrops and ask you not to touch your eye. I then put a dye which stains your tears yellow. And then I check your eye pressures under blue light on the slit lamp, with a prism that comes close to the eye.
It takes less than a minute if you don’t blink and keep looking straight ahead, and a few extra seconds if you fidget. It’s painless, and quick, and we finish with a drop of antibiotic in the eye.
Step 4: Dilation, When It Is Needed
If your assessment requires dilating your pupils, you will be told this in advance, because dilation takes about forty five minutes to take full effect and changes how you experience the rest of your day.
We ask you to bring dark glasses, a scarf, or an umbrella, since dilated eyes are far more light sensitive, particularly in Gurugram’s daytime heat
We advise you not to drive yourself home after a dilated examination
Step 5: Establishing a True Baseline, Not a Single Snapshot
Glaucoma decisions should never rest on one reading taken on one day. Two specific habits in my clinic exist to correct for that.
Repeating your first visual field
There is a genuine learning curve to taking a visual field test well. The first attempt is frequently unreliable simply because the patient has not yet learned the rhythm of the test. I routinely discard the first visual field and ask patients to return the next morning. We do not charge for that repeat test. The inaccuracy is a known limitation of the test itself, and is not a reason to bill twice.
Three pressure readings, not one
For a true baseline, I usually take three intraocular pressure readings at different times of day. Rather than relying on a single number, since pressure naturally fluctuates through the day. One of these three readings may be taken by an optometrist, if it’s after my working hours. We usually work from the average of all three.
The water drinking test
A formal diurnal variation test, in which pressure is measured every few hours through the day, is not practical for every patient. We often use the water drinking test as a more practical stand in. This is typically done before starting treatment, again about one to two months after treatment begins. We may repeat it if your eye appears to be progressing despite your pressure meeting its target.
Step 6: Setting Your Personalised Target Pressure
There is no single universal normal pressure number in modern glaucoma care. Your corneal thickness, the structure of your drainage angle, and your Visual field and OCT baseline are combined to calculate a target pressure zone. This is specific to your eye, designed to halt progression for you.
Step 7: The Most Important Section of Glaucoma Consultation: Eye Drop Training
A prescription on its own does not protect your vision if the drops never go in correctly or are forgotten. So every consult ends with practical training, not just instructions.
I personally show you how to instil your eye drops correctly, since technique affects how much medication actually reaches the eye
I ask you to set a phone alarm for every dose. Because relying on memory alone is the most common reason treatment fails
If you are on more than one medication, I recommend keeping two small boxes. One empty and one full of your drop bottles. After each dose, you move that bottle from the full box to the empty one. So a glance at the boxes tells you whether you have already taken that round of drops. And which ones remain.
When you leave, my coordinator helps you set your next appointment, before you leave the clinic. You will also receive a Whatsapp message with links to important information and details of phone numbers to book appointments. You will also get my direct phone number for any clinical queries, or emergencies.
When To See Me Before Your Booked Glaucoma Consultation
Sudden eye pain, redness, or blurred vision, which can signal an acute angle closure attack
Any one sided change in vision or eye appearance
Headache or nausea accompanying eye pain
A noticeable change in your visual field between scheduled visits
New side effects after starting or changing a glaucoma medication
Missed doses for several consecutive days, which should be flagged at your next visit rather than left unmentioned
Why does the optometrist see me before the doctor does?
The optometrist’s workup, history, refraction, and the three part vision check, ensures your file is complete and your baseline vision is documented accurately before I begin my own examination. This makes the time I spend with you more focused on interpretation and decision making rather than data collection.
Why do you measure my eye pressure yourself instead of leaving it to staff?
Goldmann applanation tonometry is the gold standard pressure test, and for every glaucoma patient I treat, I perform it myself before starting treatment, at the first follow up, and at every annual review. It gives me a direct sense of your eye’s behaviour that I do not want to lose by always delegating it.
Why do you discard my first visual field test and ask me to repeat it?
Most patients have not yet learned the rhythm of the visual field test on their first attempt. This makes that first result unreliable. We ask you to return the next morning for a repeat test. We do not charge for it, since the inaccuracy belongs to the learning curve of the test, not to you.
Why is gonioscopy done after OCT and visual field testing, not before?
When OCT, visual field testing, and fundus photography are part of your visit, I prefer to have that structural and functional picture in hand before manipulating the angle during gonioscopy. The order is chosen to give the cleanest possible baseline. Also, sometimes I use a viscoelastic gel for gonioscopy. In that case, your vision is fuzzy for about ten minutes after, and I don’t want your time wasted.
What is the water drinking test and why would I need one?
It is a practical way of checking how your eye pressure responds to a physiological stress. This is used in place of round the clock diurnal variation testing, which is not feasible for every patient. I typically use it before starting treatment. I may repeat it again a month or two into treatment. And again later if your eye appears to be progressing even though your pressure looks controlled.
Why do you spend time teaching me to put in my own eye drops?
Technique directly affects how much medication reaches your eye. A missed or mistimed dose is the most common reason glaucoma treatment underperforms. Pairing a phone alarm with the two box system is simple. It gives you a simple, visual way to know whether today’s dose has already gone in. Research says it is the most important intervention in preventing glaucoma blindness.
Key Takeaways
Your consult begins with the optometrist. They document history and perform three vision measurements, UCVA, PGP, and BCVA, before I examine you
Testing follows a fixed order: imaging and visual field first when needed, then corneal thickness, then gonioscopy, then pressure measurement
I personally measure your eye pressure for every glaucoma patient at key visits, rather than delegating it
Your first visual field is usually repeated free of charge, because of a genuine learning curve with the test
Baseline pressure is built from three readings at different times of day, sometimes supplemented by a water drinking test
Your target pressure is personalised to your eye’s anatomy, not based on one generic normal number
No consult ends without hands on training in how to use your drops. And how to track whether you have taken them
Book a Consultation
If you have been told you have glaucoma, or are due for a routine check because of family history or elevated pressure, this is the process you can expect to walk through.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Glaucoma vision is often described as gradually losing side vision, making it harder to notice objects, navigate spaces, or see hazards. Because early glaucoma rarely causes symptoms, regular eye examinations are essential for early detection. Glaucoma usually develops slowly and painlessly, often affecting peripheral (side) vision before central vision. Many people do not notice symptoms until significant and irreversible vision loss has already occurred.
Glaucoma vision does not feel like anything in its early stages. That is the defining and most dangerous feature of this disease. By the time most people notice something is wrong, significant and permanent nerve damage has already occurred.
What Glaucoma Vision Actually Feels Like at Every Stage
Most eye diseases announce themselves. Glaucoma does not. It is a disease of gradual, silent loss, and the experience of that loss is unlike almost anything else in medicine.
Understanding what glaucoma vision feels like at each stage helps you recognise warning signs earlier, take monitoring seriously, and explain your experience accurately to your doctor.
Early Glaucoma: You Feel Nothing
In early glaucoma, peripheral vision begins to fail. The optic nerve loses fibres quietly. No pain, no redness, no blur. Your brain fills in the gaps using information from your other eye and from past visual experience. This is called neural compensation.
You do not see a black patch. You see nothing wrong. Your brain edits the missing information out of your awareness before you ever become conscious of it. This is why early glaucoma is genuinely invisible to the person who has it.
The only reliable way to detect early glaucoma is through examination. Intraocular pressure measurement, optic nerve imaging, and visual field testing reveal damage that the patient cannot feel and cannot describe.
Moderate Glaucoma: The Gaps Begin to Appear
As glaucoma progresses, the areas of lost vision become larger. They can no longer be hidden by neural compensation alone. Patients at this stage describe experiences that are specific and worth knowing.
Missing patches that are hard to locate. Not seeing a dark spot. You miss things that were there. You reach for a glass and it is not where you expected. In fact, you may step off a kerb without seeing it. You lose track of a word while reading and cannot find your place again.
Difficulty in crowds. Faces appear and disappear unexpectedly. People seem to emerge from nowhere because they entered your visual field through an area that no longer reports properly.
Trouble on stairs and uneven ground. Depth perception requires full peripheral vision. When peripheral fields narrow, steps become harder to judge. Falls become more likely.
Slower recovery in dim light. Many patients notice that moving from a bright space to a dim one takes longer than it used to. Glaucoma damages the cells responsible for low-light sensitivity earlier and more severely than those handling bright light.
Glare sensitivity. Headlights, sunlight on water, and bright screens can feel more uncomfortable than before. This is partly nerve damage and partly the effect of raised intraocular pressure on the optical media of the eye.
Advanced Glaucoma: Tunnel Vision
In advanced disease, the visual field contracts severely. Patients describe this as looking through a narrow tube or pipe. Central vision remains sharp because the macula is often the last area affected. Patients can still read and recognise faces. But they cannot see what is beside, above, or below them.
This creates a profound and specific disability. Reading is possible. Walking safely is not. Driving is impossible. Navigating a room without knocking into furniture is a daily challenge. The disconnect between intact central vision and devastated peripheral vision confuses people who do not understand glaucoma. A patient may appear to see perfectly while being functionally blind for most activities of daily life.
End-Stage Glaucoma and Blindness
End-stage glaucoma results in the loss of central vision as well. The patient may retain light perception or hand motion vision. Full blindness from glaucoma is total loss of all functional sight. It is permanent. No treatment restores vision that glaucoma has destroyed.
This is the core clinical reality that shapes everything in glaucoma management. The damage is irreversible. The goal is always to stop further loss, not to recover what is gone.
Acute Angle-Closure Glaucoma: A Different Experience Entirely
The descriptions above apply to primary open-angle glaucoma, which is the most common type. Acute angle-closure glaucoma is different and dramatic.
In acute angle closure, intraocular pressure rises suddenly and severely. The experience is unmistakable. Patients describe intense eye pain, a headache centred around the eye and brow, nausea, vomiting, and vision that becomes blurred and hazy. They often see rainbow-coloured halos around lights. The eye becomes red. The cornea looks hazy even to an observer.
This is a medical emergency. It requires treatment within hours to prevent permanent vision loss. If you or someone you know experiences these symptoms, seek emergency eye care immediately.
Understanding Symptoms & Signs
Glaucoma Stage
What the Patient Experiences
What Standard Vision Tests Show
Early
Nothing. No symptoms.
Normal acuity, subtle optic nerve changes, early field defect on testing
Moderate
Missing objects, misjudging steps, difficulty in crowds
Reduced peripheral field on formal perimetry
Advanced
Tunnel vision, frequent falls, cannot drive
Severely constricted visual field, preserved central acuity
End-stage
Near or complete blindness
Central field loss, minimal or no functional vision
Patients with moderate to advanced glaucoma frequently pass standard vision chart tests with flying colours. A 6/6 Snellen result means your central vision is intact. It says nothing about your peripheral field. Doctors, family members, and even some healthcare professionals mistake a good acuity reading for good overall vision.
This misunderstanding has real consequences. Patients are told they see well when they cannot drive safely, cannot walk without risk, and cannot function independently. Visual acuity and visual field are two separate measurements. Both matter. In glaucoma, the field is the critical one.
What to Do If You Recognise These Descriptions
If what you have read here sounds familiar, act now. Glaucoma is treatable. Vision lost cannot be recovered, but further loss can almost always be stopped or slowed significantly with the right intervention.
You need a formal visual field test, an optic nerve assessment with imaging, and an accurate intraocular pressure reading taken at the right time of day. If you have already been diagnosed and your symptoms are progressing, your current treatment may not be sufficient.
A specialist opinion is not a sign that something has gone wrong. It is the most responsible thing you can do for your long-term vision.
Primary open-angle glaucoma, the most common type, causes no pain at any stage. Pain is a feature of acute angle-closure glaucoma, which is a different condition requiring emergency treatment. The absence of pain in open-angle glaucoma is precisely why it is so often diagnosed late.
Can you see the blind spots caused by glaucoma?
No. The brain fills in missing areas of visual field automatically. You do not see black patches. You simply fail to see things that fall in the damaged area. This is why patients are genuinely unaware of early and even moderate field loss.
Is glaucoma vision loss different in both eyes?
Usually, yes. Glaucoma typically progresses at different rates in each eye. The better eye compensates for the worse one. This further masks the degree of real vision loss until the disease is quite advanced in at least one eye.
How fast does glaucoma vision loss progress?
Rate of progression varies widely. Some patients lose very little vision over decades. Others progress quickly despite treatment. Pressure control, disc structure, blood flow, and genetic factors all play a role. This is why ongoing monitoring matters as much as the initial treatment decision.
Can glaucoma vision loss be reversed?
No. Optic nerve fibres that glaucoma destroys do not regenerate. Current treatment preserves remaining vision by controlling intraocular pressure and, where possible, protecting the optic nerve. Research into neuroprotection is active. There is currently no approved therapy to restore lost glaucomatous vision.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
Asymmetric focusing, where one eye is noticeably slower or less clear than the other, can indicate different prescriptions between eyes (anisometropia), early cataract in one eye, or asymmetric glaucoma or AMD. Asymmetry in vision symptoms should always be evaluated promptly.
You cover one eye and things look clear. You switch to the other and there is a moment of blur, or the image never quite sharpens to the same degree. The difference might be subtle: you notice it reading signs, switching between near and far, or in low light.
Symmetry in vision between the two eyes is expected. When it changes, especially in one direction, something has changed in that eye. It is worth finding out what.
One eye is more short-sighted, long-sighted, or astigmatic than the other. Common and correctable, but can cause strain if uncorrected.
Early cataract
Lens clouding reduces contrast and sharpness in that eye. Focusing becomes effortful and less crisp.
Asymmetric dry eye
The tear film is less stable in one eye, causing intermittent blurring and focusing lag.
Early glaucoma (asymmetric)
Glaucoma frequently begins in one eye before the other. Reduced contrast sensitivity in that eye can present as asymmetric visual quality.
Amblyopia (lazy eye)
If one eye developed poor vision in childhood without correction, this manifests as persistent asymmetry in adult visual function.
Corneal irregularity
Surface changes in one eye distort focus without reducing standard measured acuity significantly.
FAQs
Is It Normal for One Eye to Focus More Slowly Than the Other?
Occasional, mild differences in focusing speed between the two eyes can be normal, especially with fatigue or after prolonged screen use. But if one eye consistently takes noticeably longer to sharpen an image, or if this is new, it warrants a proper examination. The eye that lags may have a refractive error, early cataract, optic nerve issue, or neurological cause that has not yet been identified.
Is Asymmetric Focusing a Sign of Glaucoma?
It can be. Glaucoma frequently causes asymmetric damage — one optic nerve is affected earlier or more severely. Patients may first notice this as one eye that feels less reliable, less sharp, or slower to adapt to changing light levels. Standard vision tests may still show 6/6 in both eyes while significant nerve damage has already occurred. This is why optic nerve imaging matters.
Can Glaucoma Cause One Eye to Focus Differently?
Glaucoma does not directly affect the focusing mechanism of the eye. But advanced glaucoma can reduce contrast sensitivity and dim overall visual quality in the affected eye, which patients sometimes describe as sluggish or slow focusing. If one eye has more glaucoma damage than the other, the visual experience in that eye will feel qualitatively different even when the prescription is the same.
Could This Be an Early Sign of a Cataract?
Yes. A cataract developing in one eye before the other is one of the most common reasons for asymmetric visual quality. The clouding of the lens affects how quickly and clearly the eye can resolve an image, particularly in changing light conditions. Patients often notice it first when switching between bright and dim environments, or when reading fine print. A slit-lamp examination will confirm it.
What Is the Connection Between Focusing Problems and the Optic Nerve?
The optic nerve carries visual information from the retina to the brain. Disease or inflammation affecting the optic nerve, including optic neuritis, glaucoma, and compressive lesions, can alter how an eye perceives and processes visual input. Patients sometimes describe this not as blurring but as a lag, a dimness, or a sense that the image in one eye is slightly behind the other. This pattern should always be investigated promptly.
When Should I See a Specialist Rather Than My Optician?
See a specialist if the difference between your two eyes is new, worsening, or accompanied by any other symptom — pain behind the eye, colour desaturation in one eye, headache, or any peripheral vision change. An optician can check your prescription and screen for obvious causes, but a full evaluation of the optic nerve, visual fields, and retina requires a specialist. Do not assume a new asymmetry between the eyes is a prescription problem until it has been properly assessed.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.