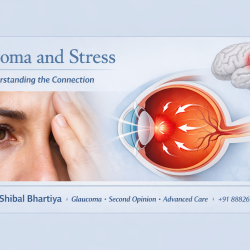
Glaucoma is the most common cause of irreversible blindness in India, and 90% of cases remain undiagnosed. That means nine out of every ten people with glaucoma in this country do not know they have it. An estimated 11.2 million Indians aged 40 and above have glaucoma. And angle closure glaucoma is more common in India, than in the West, says Dr Shibal Bhartiya. Glaucoma in India is often missed or undertreated because it progresses silently, even when vision and eye pressure appear normal. Good glaucoma care focuses on early detection, risk-based monitoring, and long-term protection of vision, not just adding more eye drops.
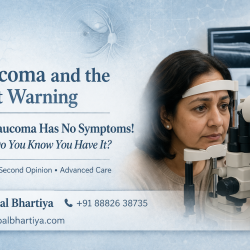
Glaucoma does not give you a warning. You lose peripheral vision first. By the time you notice something is wrong, damage is already done. The good news is that glaucoma detected early is highly manageable. Blindness from glaucoma is largely preventable with timely diagnosis and consistent treatment.
In India, this story plays out every day at a scale that is hard to comprehend. Dr Shibal Bhartiya, fellowship trained glaucoma specialist in Gurgaon, explains more about Glaucoma in India, and Indians.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Why Indians Are at Higher Risk
Indians carry specific anatomical and genetic traits that raise their glaucoma risk. One of the most significant is a shallower anterior chamber angle. This makes angle-closure glaucoma far more common in Indian and South Asian eyes than in Western populations.
Primary angle-closure disease may affect as many as 27.6 million Indians. Patients with primary angle-closure glaucoma are twice as likely to go blind compared to those with open-angle glaucoma. Yet this form is frequently missed or misdiagnosed.
Indians also present with glaucoma at a younger age than patients in Western populations. Juvenile open-angle glaucoma, which begins between the ages of 16 and 40, is well documented in Indian tertiary centre data. A family history of glaucoma raises your personal risk significantly. If a parent or sibling has glaucoma, your chances of developing it are much higher.
Other risk factors specific to the Indian context include:
Steroid use without medical supervision, myopia (short-sightedness), diabetes, and a family history of glaucoma are all important risk factors to discuss with your doctor.
The Problem of Late Presentation
Most glaucoma in India is detected late. Very late.
In India, undetected and untreated glaucoma leads to faster progression, earlier visual impairment, and preventable blindness. The core reason is that glaucoma causes no pain and no blur in the early stages. People feel completely fine. They see no reason to visit an eye doctor.
By the time central vision is affected, up to 90% of peripheral nerve fibres may already be lost. That damage cannot be reversed. No surgery, no medication, and no intervention brings that vision back.
This is what makes early screening so critical. You cannot feel glaucoma coming. You can only catch it on examination.
The Scale of the Problem in India
Glaucoma prevalence among Indians aged 40 and above ranges between 2.7% and 4.3% across multiple population-based studies. In those over 70 years of age, the risk rises sharply. Studies show glaucoma affects over 8% of Indians in their seventies and over 14% of those above 80.
Glaucoma is a leading cause of irreversible blindness globally, and the burden in Asia and India is expected to grow substantially by 2040.
India does not have enough glaucoma specialists to manage this burden. Most patients are diagnosed and managed by general ophthalmologists. Structured, specialist-led care makes a real difference to outcomes.
What Makes Glaucoma in Indians Different to Manage
Treating glaucoma in an Indian patient requires a different approach than using a standard Western protocol.
Indian eyes tend to have thinner corneas. Corneal thickness affects how accurately we measure intraocular pressure (IOP). A thin cornea can make the pressure appear lower than it actually is. This leads to underdiagnosis and undertreatment. Also, thinner corneas are an independent risk factor for glaucoma progression.
Angle-closure disease needs gonioscopy, a specialised examination to assess the drainage angle of the eye. Studies have found that a significant proportion of patients in India are incorrectly treated for open-angle glaucoma when they actually have angle-closure disease.The treatment for these two types is fundamentally different.
Normal tension glaucoma (NTG), where optic nerve damage occurs despite normal eye pressure, is also seen in Indian patients. This form requires looking beyond IOP and addressing other risk factors including blood pressure, sleep patterns, and vascular health.
How I Approach Glaucoma in Indian Patients
I have spent 25+ years specialising in glaucoma. I see this disease in its full Indian context, not through a textbook written for another population.
My clinical approach includes a full angle assessment with gonioscopy for every new patient, corneal thickness measurement to ensure accurate pressure readings, structural imaging with OCT to detect early nerve fibre loss, visual field analysis (with special emphasis on reliability criteria) and a detailed risk factor review including family history, steroid use, and systemic health.
Correct classification, open-angle versus angle-closure, changes treatment completely. Getting this right at the first visit prevents years of inadequate care.
I also believe in clear communication. Glaucoma is a lifelong condition. You need to understand what you have, why treatment matters, and what to monitor. I take the time to explain this at every visit.
If you have a family history of glaucoma, are over 40, have diabetes, are short-sighted, or use steroid eye drops, you need a glaucoma screening now.
Clinical Reality (What’s Not Always Obvious in Glaucoma Care in India)
- Normal vision does not mean no glaucoma
Many patients read 6/6 and still have significant optic nerve damage. - Symptoms are often absent until late
Glaucoma is typically silent — by the time patients notice vision loss, it is often irreversible. - Eye pressure (IOP) alone is not enough
Patients can progress despite “normal” pressures — especially in normal-tension glaucoma, which is common in India. - Tests in isolation can mislead
A single OCT or visual field report cannot define disease. Progression over time is what matters. - Cataract and glaucoma often coexist — but are not interchangeable explanations
Improving vision after cataract surgery does not mean glaucoma risk is gone. - More medications ≠ better control
Multiple drops without a clear long-term plan often reflect escalation without strategy. - Follow-up gaps are a major cause of vision loss
Irregular monitoring is one of the biggest real-world failures in glaucoma care. - Family history is under-recognised and under-screened
Many high-risk individuals in India are never examined until damage has already occurred.
What Good Glaucoma Care Looks Like (Indian Context)
- Early risk identification — even before symptoms
Screening is guided by age, family history, corneal thickness, optic nerve appearance — not just complaints. - Baseline documentation and longitudinal tracking
OCT and visual fields are used to establish a baseline and detect change, not just diagnose once. - Target pressure is individualised
Treatment is tailored based on stage of disease, risk profile, and rate of progression — not a fixed number. - Medication strategy is structured, not reactive
Each drop has a purpose. Escalation is thoughtful, not additive. - Patient understanding is prioritised
Patients are told what to watch for: subtle visual changes, adherence issues, side effects. - Consistency over intensity
Regular follow-up (every 3–6 months depending on risk) matters more than aggressive but irregular care. - Second opinions are used appropriately
Especially when:- Disease is progressing despite treatment
- Multiple medications are being used
- Surgery is being considered
- The goal is not just seeing clearly — but seeing safely for life
Glaucoma care is long-term risk management, not short-term vision correction.
Remember
| Situation | What Patients Often Assume | Clinical Reality (India Context) | What Good Care Looks Like |
|---|---|---|---|
| Vision is normal | “I can see clearly, so everything is fine” | Glaucoma can cause optic nerve damage even with 6/6 vision | Risk-based screening and optic nerve evaluation, even without symptoms |
| No symptoms | “No discomfort means no disease” | Glaucoma is silent until late stages | Early detection through structured exams, not symptom-driven visits |
| Eye pressure (IOP) | “My pressure is normal, so I’m safe” | Progression can occur even at normal IOP (common in India) | Individualised target IOP based on risk and progression |
| Single test reports | “My OCT/field test is normal” | One report is not enough — change over time matters | Baseline + serial comparison to detect progression |
| Cataract vs glaucoma | “Cataract surgery fixed my vision, so I’m okay” | Cataract improvement can mask underlying glaucoma | Parallel evaluation of optic nerve even in cataract patients |
| Multiple eye drops | “More drops means stronger treatment” | Overmedication may reflect lack of strategy | Structured medication plan with defined goals |
| Follow-up gaps | “I’ll come back if I feel a problem” | Irregular follow-up is a major cause of preventable vision loss | Scheduled monitoring every 3–6 months based on risk |
| Family history | “No one told me to get checked” | High-risk individuals often remain unscreened in India | Proactive screening for family members |
| Treatment approach | “Doctor will adjust if needed” | Reactive care often misses slow progression | Long-term planning with defined targets and timelines |
| Understanding disease | “Drops are enough” | Poor understanding leads to poor adherence | Clear patient education on disease, risks, and expectations |
| Escalation decisions | “Add another drop if pressure rises” | Escalation without strategy leads to confusion and side effects | Stepwise, purpose-driven escalation or de-escalation |
| Goal of care | “I just need to see clearly” | Vision clarity ≠ visual safety | Focus on lifelong preservation of functional vision |
FAQs: Glaucoma in Indians
Is glaucoma more common in Indians?
Yes. Indians face a higher risk than many Western populations for two main reasons. First, Indian eyes tend to have a shallower drainage angle, which makes angle-closure glaucoma significantly more common. Second, glaucoma in Indians often develops at a younger age and is detected later, by which time substantial nerve damage has already occurred.
Can Indians get glaucoma even with normal eye pressure?
Yes. Normal tension glaucoma (NTG) occurs when the optic nerve is damaged despite intraocular pressure readings within the normal range. This form is well documented in Indian patients. It is one reason why pressure measurement alone is not enough. A full glaucoma evaluation includes optic nerve imaging and visual field testing.
What are the early signs of glaucoma in Indians?
In most cases, there are no early signs. Glaucoma is called the silent thief of sight because it causes no pain and no blurred vision until the disease is advanced. Peripheral vision goes first, and most people do not notice this until significant damage has occurred. The only reliable way to detect early glaucoma is a comprehensive eye examination.
Who should get screened for glaucoma in India?
Anyone over 40 should have a baseline glaucoma check. Screening is especially important if you have a family history of glaucoma, are short-sighted, have diabetes, use steroid eye drops, or have previously been told your eye pressure is elevated. Earlier screening is recommended if more than one risk factor applies.
How is glaucoma treated in Indian patients?
Treatment depends on the type of glaucoma. Angle-closure glaucoma, which is more common in Indians, often requires laser treatment (laser peripheral iridotomy) in addition to or instead of eye drops. Open-angle glaucoma is typically managed with pressure-lowering drops, laser, or surgery. The right treatment must be matched to the specific type of glaucoma you have, which is why correct diagnosis through gonioscopy and full assessment is essential.
If you have been told you have glaucoma but have not had gonioscopy or a visual field or OCT imaging, a structured second opinion can clarify your diagnosis and treatment plan.
Book a consultation with Dr Shibal Bhartiya:
Marengo Asia Hospitals, Gurugram
Phone: +91 88826 38735
Website: drshibalbhartiya.com
Google Business Profile: maps.app.goo.gl/mcfegmHTuhqV5hSp6
Read the research articles
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. This article was updated in May 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks, span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Available on Pubmed and Google Scholar
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
Patient reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma