Untreated glaucoma causes permanent, irreversible vision loss, and in most cases, patients feel nothing until significant damage has already occurred. Glaucoma destroys the optic nerve silently. By the time you notice a change in your vision, up to 40% of nerve fibres may already be gone, explains Dr Shibal Bhartiya.
Many people discover glaucoma late because it causes no pain, no redness, and no early warning signs in its most common form. That silence is what makes it dangerous. If you have been told your eye pressure is high, or if glaucoma runs in your family, the question of what happens if you leave it alone is not academic. It is urgent.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
7 Things That Happen When Glaucoma Goes Untreated
1. The Optic Nerve Keeps Deteriorating
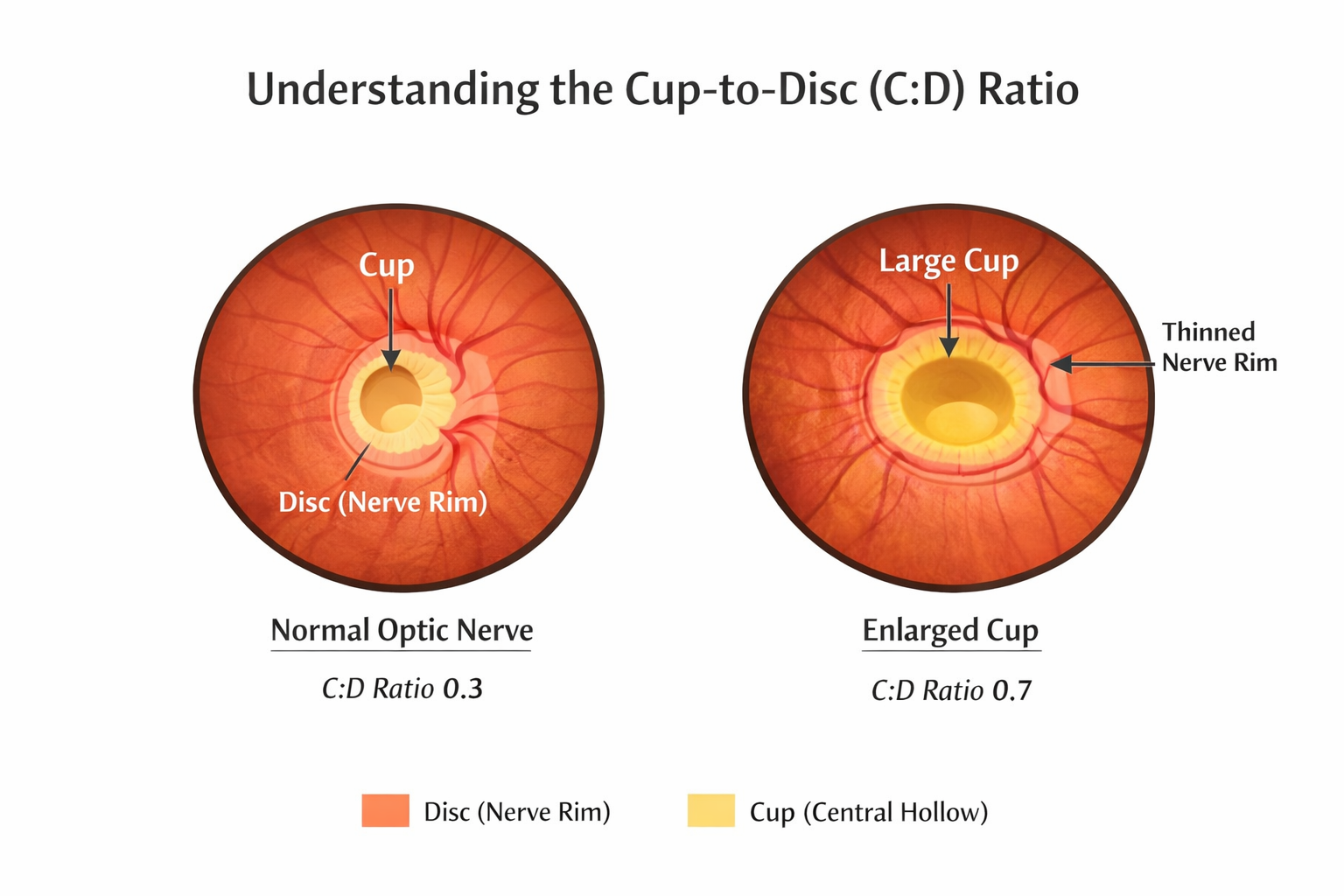
Glaucoma damages the optic nerve, the cable that sends visual signals from your eye to your brain. Each day without treatment, elevated pressure continues to compress and starve nerve fibres of blood supply. Once a nerve fibre dies, it does not regenerate. There is no surgery, no medication, and no natural process that restores it.
Treatment slows or stops this process. No treatment means no brake on the damage.
2. Peripheral Vision Disappears First
The first field of vision to go is your peripheral vision, the edges of what you see. This happens so gradually that most patients do not notice. The brain fills in the gaps, masking the loss. You may be losing significant side vision for years before you register anything unusual.
By the time you notice you are bumping into things, misjudging doorframes, or struggling to see cars approaching from the side, the damage is already extensive.
3. Central Vision Is Eventually Affected
A common misconception is that glaucoma only affects side vision and central vision stays intact. This is true in early and moderate stages, but untreated glaucoma progresses. As more of the optic nerve is destroyed, the visual field loss closes in from the edges toward the centre. At advanced stages, the remaining central tunnel of vision narrows severely.
At end-stage glaucoma, even central vision is lost.
4. Blindness Becomes a Real Risk
Glaucoma is the leading cause of irreversible blindness worldwide. It is the number one cause of preventable blindness in India. The word “preventable” matters, because the blindness is not inevitable. It is the outcome of late diagnosis or no treatment.
Patients who are diagnosed early and treated consistently rarely go blind from glaucoma. Patients who ignore it, or who stop treatment because they feel well, are the ones who lose vision permanently.
5. Acute Angle-Closure Can Cause Sudden Blindness
Not all glaucoma is slow and silent. Acute angle-closure glaucoma is a medical emergency. Eye pressure spikes suddenly and severely. Patients experience intense eye pain, headache, nausea, vomiting, and blurred vision with coloured halos around lights.
If this is not treated within hours, it can cause permanent blindness in that eye. Many patients mistake it for a migraine or food poisoning and delay seeking care. This delay can cost them their sight.
6. Quality of Life Declines Significantly
Vision loss from untreated glaucoma is not just a medical number on a visual field report. It changes how you live. Driving becomes unsafe, then impossible. Reading becomes difficult. Recognising faces becomes unreliable. Falls and accidents become more frequent. Depression and anxiety are significantly more common in people with advanced glaucoma.
The impact is gradual enough that patients adapt, until they can no longer. At that point, the vision loss cannot be reversed.
7. Treatment Becomes Harder as Damage Advances
In early glaucoma, a single eye drop once daily may be all that is needed to control pressure and preserve vision. As glaucoma advances, more medications are required. Laser treatments may be needed. Surgery, with longer recovery times, higher risks, and no guarantee of reversing existing damage, becomes the only option.
Treating glaucoma early is simpler, cheaper, and far more effective than treating it late.
What Doctors Often Miss Telling Patients
Most patients are told they have high eye pressure or early glaucoma and are given drops. What they are not always told clearly is this: the drops do not make you feel better. They do not improve your vision. They work silently in the background to prevent future damage.
Because there is no immediate reward, no symptom that goes away, no vision that returns, many patients stop their drops after a few weeks. They feel the same. They assume they are fine. This is the most dangerous point in glaucoma care.
Stopping treatment does not mean the disease has stopped. It means the only thing slowing the damage has been removed.
As a glaucoma specialist, I have seen patients who were diagnosed years earlier, given drops, and told to return in six months. Life got busy. The drops ran out. The follow-up did not happen. When they finally return, sometimes years later, significant, irreversible vision loss has occurred in the interval.
This is preventable. Every time.
Symptom Progression: What to Watch For
| Stage | What You May Notice | What Is Actually Happening |
|---|---|---|
| Early | Nothing at all | Peripheral nerve fibres dying |
| Moderate | Occasional blind spots at the edges | 30–50% nerve fibre loss |
| Advanced | Bumping into objects, missing steps, tunnel vision | 70–80%+ nerve fibre loss |
| End-stage | Loss of all but a sliver of central vision | Near-total optic nerve destruction |
| Acute attack (angle-closure) | Sudden severe eye pain, headache, halos | Medical emergency — act within hours |
When Act Immediately? If You Have
- A family history of glaucoma and have never had an eye pressure check
- Been told your eye pressure is high but have not started treatment
- Started treatment but stopped because you felt no difference
- Not had a visual field test or OCT scan in more than a year
- Sudden eye pain, nausea, and blurred vision with halos
What This Means for You
Glaucoma is manageable. That is the truth that often gets lost in the fear around the diagnosis. The vast majority of patients who are diagnosed early, treated appropriately, and followed up consistently do not go blind. They live full, visually intact lives.
But glaucoma does not forgive neglect. It does not pause when life gets busy. It does not announce its progress. The only protection is a specialist who checks, measures, and adjusts your treatment over time, and a patient who shows up.
If you have been diagnosed with glaucoma, or if someone in your family has it, a comprehensive glaucoma evaluation is not something to delay. The damage happening right now is silent. The window to prevent it from becoming permanent is open, but it does not stay open forever.
Frequently Asked Questions
Can glaucoma be reversed if caught early?
The nerve damage already present cannot be reversed. However, early treatment stops further damage from occurring. Patients diagnosed early and treated consistently typically keep their functional vision for life.
Is it safe to stop glaucoma drops if I feel fine?
No. Glaucoma drops prevent damage, they do not treat symptoms, because there are none. Feeling well means the drops are working. Stopping them removes the only thing protecting your optic nerve.
How fast does untreated glaucoma progress?
This varies by type and individual. Some patients progress slowly over decades; others, particularly those with very high pressures or angle-closure glaucoma, can lose significant vision within months or years. There is no way to predict your rate without regular monitoring.
What is the difference between glaucoma suspects and glaucoma?
A glaucoma suspect has risk factors: high pressure, suspicious optic nerve appearance, or a family history, but no confirmed nerve damage yet. This group needs careful monitoring, as some will develop glaucoma. Not all glaucoma suspects need treatment, but all need regular follow-up.
Can I drive if I have glaucoma?
In early and moderate glaucoma, most patients can drive safely. In advanced glaucoma with significant peripheral field loss, driving may be unsafe and may not meet legal vision standards. This should be assessed with a formal visual field test.
Should You See a Glaucoma Specialist?
If you have been diagnosed with glaucoma, suspect you may have it, or have a parent or sibling with the condition, a specialist evaluation gives you information a general eye check cannot.
A glaucoma specialist will assess your optic nerve in detail, measure your visual field, perform OCT scanning of the nerve fibre layer, and build a personalised treatment and monitoring plan. The goal is not just to lower your eye pressure. The goal is to protect your vision for the rest of your life.
Book a glaucoma consultation at Marengo Asia Hospitals, Gurugram.
📞 +91 88826 38735 | 🌐 www.drshibalbhartiya.com
Upload your previous reports for a second opinion, a fresh set of expert eyes on your case can change the outcome.
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma