Two patients. Same diagnosis. Similar eye pressure. Same drops. One is stable at ten years. The other has lost significant…
Tag: glaucoma progression risk factors
When Glaucoma Keeps Progressing
Glaucoma can progress even with treatment. The most common reasons include suboptimal IOP control, non-adherence to drops, normal-tension progression, and unrecognised structural risk factors. Finding the cause and adjusting treatment early can prevent further vision loss, says Dr Shibal Bhartiya.
Glaucoma progresses in some patients despite regular treatment. This does not mean the treatment has failed, it means the treatment plan needs review.
Understanding why glaucoma advances is the first step toward stopping it. Several factors can drive progression even when eye pressure appears controlled.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
What Does Progression Mean in Glaucoma?
Progression means measurable worsening of the optic nerve or visual field over time. Specialists confirm it using two or more reliable visual field tests and OCT imaging showing thinning of the retinal nerve fibre layer.
A single abnormal test does not confirm progression. Consistent change across multiple visits does.
Why Glaucoma Progresses Despite Drops
1. Eye Pressure Is Still Too High
The target intraocular pressure (IOP) is individual. A pressure that seems normal may still be too high for a given optic nerve. Studies show that lower IOP targets reduce progression rates in moderate and advanced glaucoma significantly.
If visual fields are worsening, the current pressure target may need revision downward.
2. Drops Are Not Working as Expected
Peak pressure often occurs in the early morning, outside clinic hours. A single office reading may miss harmful pressure spikes. Diurnal IOP curves — tested over several hours — can reveal fluctuations that drive unseen damage.
3. Non-Adherence to Eye Drop Therapy
Studies using electronic monitoring show that patients use drops correctly only 50 to 70 percent of the time. Missing doses, incorrect technique, or preservative intolerance all reduce drug efficacy. Non-adherence is the most correctable cause of progression.
4. Normal-Tension Glaucoma Behaving Differently
Some patients have optic nerve damage at pressures within the normal range. This is normal-tension glaucoma (NTG). It may involve poor vascular supply to the nerve, sleep apnoea, low blood pressure at night, or other systemic factors that drops alone cannot address.
5. Structural Risk Factors Not Yet Addressed
Thin corneas cause IOP readings to appear falsely low. A myopic or tilted optic disc is harder to interpret on imaging. Disc haemorrhages are a strong marker of ongoing progression and must be documented carefully.
6. Systemic Factors Affecting the Optic Nerve
Low systolic blood pressure, anaemia, sleep apnoea, and vascular disorders can reduce blood flow to the optic nerve. Treating these conditions alongside glaucoma can slow visual field loss in susceptible patients.
| Reason for Progression | What It Means | Next Step |
| IOP target not low enough | Nerve still under excess pressure | Lower target IOP or add therapy |
| Pressure spikes between visits | Diurnal fluctuation causing damage | Diurnal IOP curve or 24-hour monitoring |
| Drop non-adherence | Inconsistent pressure lowering | Technique review, preserve-free drops, fixed combos |
| Normal-tension glaucoma | Vascular or non-pressure mechanism | Systemic workup, cardiology review |
| Thin cornea or high myopia | IOP underestimated by tonometry | Corneal-corrected IOP, adjusted targets |
| Disc haemorrhage | Active ischaemia at optic nerve | Close follow-up, often signals rapid progression |
| Systemic comorbidity | Poor vascular supply to nerve | Treat sleep apnoea, anaemia, hypotension |
When to Consider Laser or Surgery
If maximum tolerated medical therapy does not achieve the revised IOP target, laser trabeculoplasty (SLT) or surgery becomes necessary. Selective laser trabeculoplasty is effective in open-angle glaucoma and can reduce the drop burden significantly.
Minimally invasive glaucoma surgery (MIGS) procedures such as iStent and iStent inject offer an option for mild to moderate glaucoma with lower surgical risk. Trabeculectomy remains the benchmark for advanced disease requiring very low pressures.
Dr Shibal Bhartiya’s published research includes peer-reviewed work on 24-hour IOP monitoring and diurnal pressure fluctuation: one of the most under-recognised drivers of progression in treated glaucoma. She has co-authored guidelines on surgical decision-making when medical therapy fails to halt optic nerve damage. As Clinical Director of Ophthalmology at Marengo Asia Hospitals, Gurugram, she manages complex progression cases with a structured protocol: reassess the IOP target, confirm adherence, evaluate vascular and systemic risk, and escalate to laser or surgery when the nerve continues to lose ground.
How Often Should You Be Reviewed?
Patients with progressing glaucoma need more frequent review — often every three to four months. Visual fields should be repeated at least four times a year if progression is suspected. OCT of the optic nerve head and RNFL should accompany each visit.
Waiting six or twelve months between visits when progression is active is not safe practice.
The Role of a Second Opinion
Glaucoma management decisions are complex. If your visual fields continue to worsen, a second opinion from a fellowship-trained glaucoma specialist adds value. Fresh eyes on your imaging, IOP pattern, and structural data can identify a missed cause.
Bringing your previous visual fields, OCT scans, and medication list to the consultation helps the specialist assess the rate of change accurately.
Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides trusted second opinions for patients seeking clarity before major treatment decisions. Both, in person, and online.
Frequently Asked Questions
Can glaucoma progress even with normal eye pressure?
Yes. Normal-tension glaucoma progresses at IOP readings within the statistical normal range. The optic nerve in these patients is more sensitive to pressure or more dependent on blood supply. Treatment often involves additional systemic assessment alongside IOP lowering.
How do I know if my glaucoma is progressing?
Your specialist tracks visual field tests and OCT scans over time. Progression is confirmed when two or more reliable tests show consistent worsening. You may not notice early progression — which is why regular monitoring matters.
What pressure should I aim for if my glaucoma is progressing?
The target varies by disease severity and rate of progression. Advanced or rapidly progressing glaucoma typically requires a target below 12 mmHg. Your specialist calculates this based on your structural damage and life expectancy.
Are there lifestyle changes that help slow progression?
Regular aerobic exercise, avoiding head-down positions such as headstands, good sleep hygiene, and managing vascular risk factors all support optic nerve health. Omega-3 supplementation and antioxidant nutrition are areas of ongoing research.
Is surgery the only option if drops stop working?
Not always. Selective laser trabeculoplasty is a non-incisional option that works well in many patients. If laser is not sufficient, MIGS procedures offer a middle path between drops and conventional surgery.
Consult a Glaucoma Specialist
If your glaucoma is progressing despite treatment, you need a specialist review, not just a medication change. The cause must be identified before the right intervention can be chosen.
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in May 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma
Related Reading
Get an Online Glaucoma Consult
Visual Field and OCT: Structure & Function Correlation
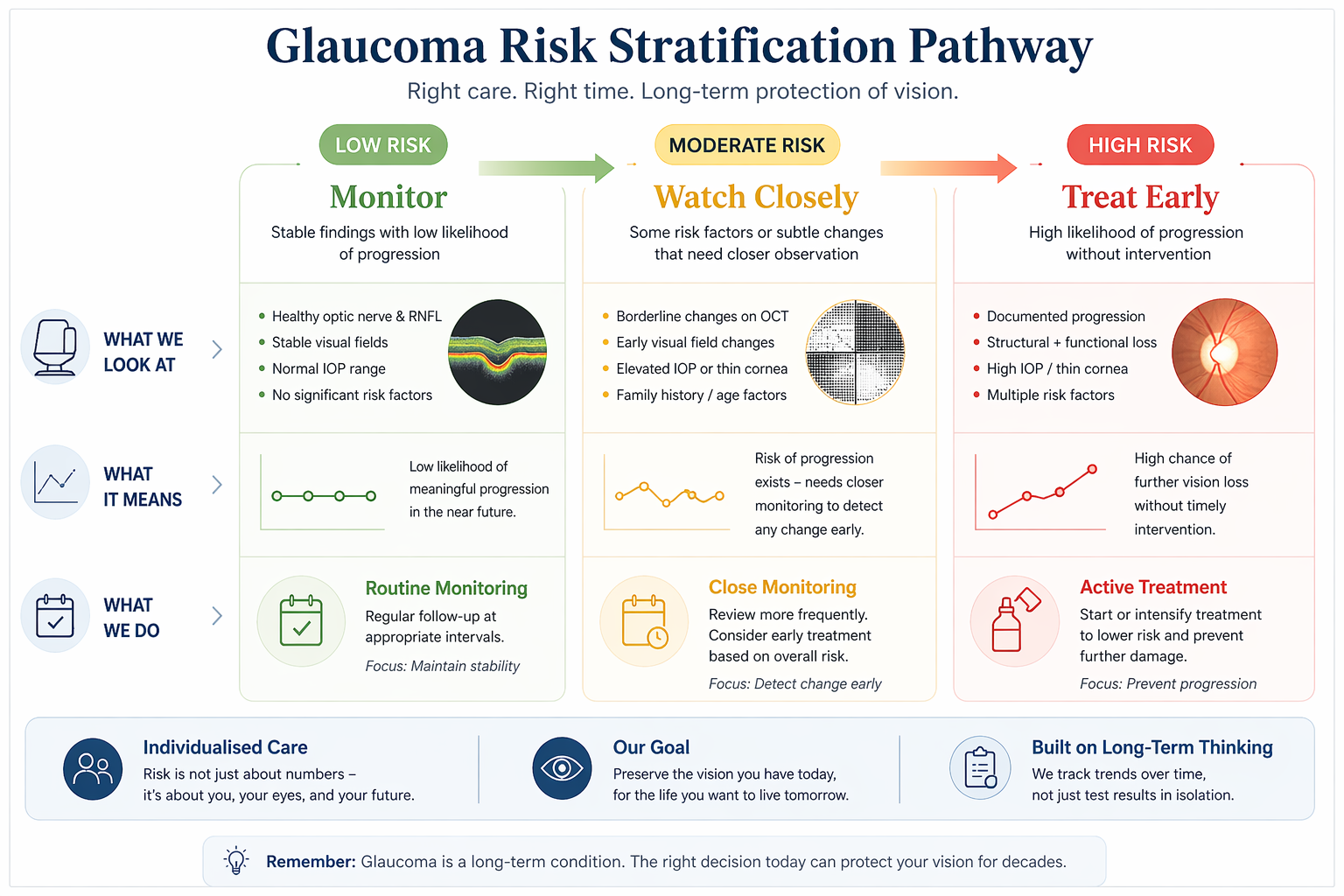
Risk Stratification in Glaucoma
Risk Stratification in Glaucoma
Risk stratification in glaucoma means assessing how likely the disease is to progress and how aggressively it should be treated. It combines optic nerve findings, eye pressure, test results, and systemic factors to guide personalised, long-term care, explains Dr Shibal Bhartiya.
Most glaucoma decisions are not about what your reports show today. They are about what your eyes are likely to do over the next 5–10 years.
Risk stratification in glaucoma helps decide who needs treatment, who can be safely monitored, and who may be at risk of silent progression, even when tests appear normal. Dr Bhartiya explains.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
🧩 WHAT THIS REALLY MEANS

Why glaucoma care is not one-size-fits-all
Two patients can have similar reports, and very different futures.
- One may remain stable for years
- Another may lose vision slowly without obvious warning
Risk stratification is the process of identifying this difference early. It helps answer the most important question:
👉 What is likely to happen if we do nothing?
⚠️WHAT MOST PEOPLE GET WRONG
Why reports alone don’t tell the full story
Many glaucoma decisions are based only on:
These are important, but incomplete.
Because:
- Structural damage can begin before symptoms
- Functional loss appears late
- Test results can fluctuate
- “Normal” does not always mean “safe”
👉 This is where many patients are either over-treated unnecessarily, or under-treated until it’s too late
🧠 HOW RISK IS ACTUALLY ASSESSED
What we look at beyond individual test results.
Risk stratification considers patterns over time, not isolated numbers.
1. Structural changes
Subtle optic nerve or OCT changes that may precede symptoms
2. Functional trends
Visual field patterns, even when still within “normal” range
3. Rate of change
How quickly (or slowly) things are evolving
4. Individual risk factors
- Family history
- Age
- Corneal thickness
- Baseline nerve health
5. Life context
How much vision loss would affect your daily function
👉 This is not just diagnosis. It is future risk prediction.
Dr Bhartiya, along with her associates, write about the current perspectives in tackling glaucoma blindness. These include raising awareness, enhancing early detection programs, and access to care, particularly in underserved populations. Pubmed.
🔍 THREE COMMON SCENARIOS
When we treat, when we monitor, and when we watch closely
🟢 Low risk
- Stable findings
- No clear progression
👉 Safe to monitor with regular follow-up
🟡 Moderate risk
- Suspicious changes
- Uncertain progression
👉 Close monitoring or early treatment depending on context
🔴 High risk
- Clear progression
- Structural + functional change
👉 Treatment is recommended to prevent further loss
👉 The goal is not to treat everyone. The goal is to treat the right patients at the right time.
⏳ THE LONG-ARC VIEW
Why early clarity matters more than late intervention
Glaucoma does not usually cause sudden symptoms. It progresses quietly. Patients may feel:
- Slight reading difficulty
- Reduced contrast
- Night discomfort
- Slower visual processing
By the time vision feels obviously affected, damage is often already established.
👉 Risk stratification in glaucoma allows intervention before this stage.
What You Must Remember
| Component | What It Means for You |
|---|---|
| Optic nerve status | Structural damage and vulnerability define baseline risk |
| Eye pressure (IOP) | Important driver, but must be interpreted in context |
| OCT findings | Early structural loss may signal higher future risk |
| Visual fields | Functional impact and progression tracking |
| Corneal thickness | Influences true pressure interpretation and risk |
| Type of glaucoma | Normal tension vs high-pressure behave differently |
| Systemic factors | Sleep apnoea, BP fluctuations, diabetes affect progression |
| Rate of change | Faster progression = higher risk category |
| Adherence to treatment | Inconsistent use increases real-world risk |
| Follow-up pattern | Regular monitoring allows timely risk recalibration |
| Big picture | Risk stratification guides target pressure, treatment intensity, and follow-up frequency |
Clinical Reality (What’s not always obvious)
Risk stratification is not about labels—it’s about deciding how closely to monitor and how aggressively to treat over time.
Risk in glaucoma is dynamic, not fixed—it changes with time, response to treatment, and systemic health.
The same eye pressure can be “safe” for one patient and damaging for another depending on optic nerve susceptibility.
Test results don’t always align—OCT, fields, and clinical exam may show different pieces of the puzzle.
Systemic factors (blood pressure dips, vascular instability, obstructive sleep apnea) can silently shift risk.
🧍♀️WHY SECOND OPINIONS MATTER HERE
When it’s worth taking a step back
You may benefit from a second opinion if:
- You’ve been advised long-term treatment without clarity
- You’ve been told to “just monitor” without explanation
- Your reports seem normal, but symptoms persist
- Your treatment keeps changing
Sometimes, the issue is not the test. It is the interpretation.
🚨 Need clarity about your glaucoma risk?
You don’t need more reports. You need to understand what they mean over time.
👉 Request a Second Opinion Consultation
Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides trusted second opinions for patients seeking clarity before major treatment decisions. Both, in person, and online.
🔎 Frequently Asked Questions
What is risk stratification in glaucoma?
It is the process of assessing how likely glaucoma is to progress over time, based on multiple factors, not just current test results.
Can glaucoma be present even if tests are normal?
Yes. Early glaucoma may not show clear changes on routine tests, especially in the initial stages.
Does everyone with glaucoma need treatment?
No. Some patients can be safely monitored, while others need early intervention depending on their risk profile.
How often should glaucoma be monitored?
This depends on individual risk. Some patients need frequent follow-up, while others can be reviewed less often.
Why do different doctors give different advice?
Because glaucoma management involves judgement, not just reports. Different interpretations of risk can lead to different recommendations.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma
Why Glaucoma Gets Worse Faster in Some People Than Others
Glaucoma can worsen faster in some people due to differences in optic nerve vulnerability, blood flow, and systemic risk factors, not just eye pressure. Even with “controlled” pressure, glaucoma may progress if underlying risks are not identified and monitored over time, Dr Shibal Bhartiya explains.
Two patients. Same diagnosis. Similar eye pressure. Same drops. One is stable at ten years. The other has lost significant field within three. Patients often ask: Why Glaucoma Gets Worse Faster in Some People Than Others.
This is not unusual in glaucoma. It is one of the most clinically important, and least explained, aspects of the disease. Your doctor told you, you have glaucoma, gave you drops. Called you back for monitoring.
But did you discuss if your optic nerve might be more vulnerable than average? Or, what factors beyond eye pressure are quietly accelerating the damage.
This article, written by Dr Bhartiya, explains those factors. Understanding them changes how glaucoma is monitored, what investigations are relevant, and what questions to ask at your next appointment.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Why Intraocular Pressure Is Only Part of the Story
The historical model of glaucoma was simple: raised intraocular pressure damages the optic nerve. Lower the pressure, stop the damage. This model is incomplete.
Intraocular pressure is the only modifiable risk factor with proven treatment benefit. It remains central to glaucoma management. But a substantial proportion of glaucoma patients, particularly those with normal tension glaucoma, progress despite pressure that is well controlled by any standard definition. And among patients with elevated pressure, some progress quickly while others with similar pressures remain stable for decades.
Pressure level explains some of the variation. The factors below explain the rest.
Central Corneal Thickness: The Hidden Pressure Modifier
Central corneal thickness (CCT) is one of the most important risk factors for glaucoma progression, and one of the most underappreciated by patients.
Intraocular pressure is measured by the resistance the cornea offers to an applanation probe or air puff. A thicker cornea gives artificially high readings. A thinner cornea gives artificially low ones. Standard Goldmann tonometry assumes a corneal thickness of approximately 545 microns. Patients with thinner corneas have their true pressure systematically underestimated at every clinic visit.
But CCT is not merely a measurement correction factor. Thin central cornea is an independent risk factor for glaucoma progression, separate from any pressure effect. The Ocular Hypertension Treatment Study (OHTS) identified CCT below 555 microns as one of the strongest predictors of conversion from ocular hypertension to glaucoma. Patients with thin corneas progress faster and reach endpoints earlier than those with normal or thick corneas, even after adjusting for measured IOP.
If you have glaucoma and have never had your corneal thickness measured, ask for it. It changes how your pressure readings should be interpreted, and it tells your specialist something important about your intrinsic risk.
Disc Haemorrhages: The Warning Signal That Gets Missed
A disc haemorrhage is a small, splinter-shaped bleed at the margin of the optic disc. It is visible on fundus examination and resolves within weeks to months. Most patients never know they have had one.
Disc haemorrhages are one of the strongest predictors of glaucoma progression. They indicate localised ischaemia, a transient interruption of blood flow, at the optic nerve head, and they mark the site of imminent or ongoing retinal nerve fibre layer loss. Studies consistently show that the sector of the optic nerve that bleeds is the sector that subsequently loses nerve fibres on OCT, and the sector where visual field loss subsequently develops.
In normal tension glaucoma, disc haemorrhages are particularly common and particularly significant. Their presence in an NTG patient is a direct signal that vascular insufficiency is active and that the nerve is under ischaemic stress beyond whatever pressure-related stress is present.
A patient whose disc haemorrhage is detected at a routine visit is not unlucky. The hemorrahe is a timely warning. The appropriate response is not to note it and move on. It is to ask why the bleed occurred, whether pressure targets need revision, and whether vascular risk factors need investigation.
Systemic Hypotension and Nocturnal Dipping
The optic nerve is supplied by blood from the posterior ciliary arteries. Like all tissues, it requires adequate perfusion pressure, the difference between arterial blood pressure and intraocular pressure, to receive oxygen and nutrients. When perfusion pressure falls, optic nerve gets less blood supply.
Systemic hypotension is a direct cause of reduced optic nerve perfusion pressure. It is most relevant at night. During sleep, blood pressure falls physiologically, this is normal nocturnal dipping. In some people, blood pressure dips excessively, by more than 20 percent from daytime levels. This is called nocturnal over-dipping.
Nocturnal over-dipping is strongly associated with glaucoma progression, particularly in normal tension glaucoma. The optic nerve, already under whatever pressure stress is present, faces additional ischaemic stress during the hours of maximum blood pressure reduction, precisely when patients are asleep and not being monitored.
The clinical implications are significant. Antihypertensive medications taken in the evening can exacerbate nocturnal dipping. A glaucoma patient who begins a new blood pressure medication and subsequently shows accelerated progression deserves a medication timing review. Taking antihypertensives in the morning rather than the evening, where clinically possible, may reduce nocturnal dipping and its consequences for the optic nerve.
A 24-hour ambulatory blood pressure monitor is a simple, non-invasive investigation that identifies nocturnal dipping. In standard glaucoma management, doctors forget about night time BP. In any patient with normal tension glaucoma or unexplained progression, however, it is essential.
Sleep Position: The Factor Nobody Mentions
The side on which a patient sleeps affects their intraocular pressure. This is documented, reproducible, and almost never discussed.
IOP is higher in the dependent eye, the eye facing down, when lying on one side. The mechanism involves increased episcleral venous pressure from the gravitational position. For a patient who sleeps consistently on one side, the dependent eye is exposed to elevated pressure for six to eight hours every night. Entirely outside the window of clinic measurement.
Studies using continuous IOP monitoring have shown that the dependent eye IOP during sleep can be 3 to 6 mmHg higher than the fellow eye. This is a clinically significant asymmetry in a disease. Especially where even 1 mmHg differences in pressure can result in measurable differences in progression rates.
This is relevant for any patient with asymmetric glaucoma, where one eye is worse than the other despite similar measured IOPs. If the worse eye is consistently the dependent eye, sleep position may be contributing.
Head-of-bed elevation, raising the head of the bed by 20 to 30 degrees, may reduce nocturnal IOP in both eyes. It is a simple, free, non-pharmacological intervention with evidence behind it.
Myopia: The Optic Nerve That Was Already Vulnerable
High myopia, short-sightedness above minus 3 to 5 dioptres, is an independent risk factor for glaucoma and for faster progression. The mechanism involves the structural anatomy of the myopic eye.
In a myopic eye, the scleral canal through which the optic nerve exits, the lamina cribrosa, is tilted, stretched, and biomechanically weaker than in an emmetropic eye. This altered geometry means the optic nerve is more susceptible to the same level of intraocular pressure that a normal eye would tolerate well. The lamina cribrosa in a myopic eye bends and deforms at lower pressure thresholds.
Myopic eyes also have thinner retinal nerve fibre layers at baseline: not from glaucoma, but from the axial elongation that stretches the retina. This makes OCT interpretation more complex: the baseline is lower, so the threshold for detecting abnormality shifts, and early glaucomatous loss can be masked within the range of normal myopic variation.
A highly myopic patient with glaucoma requires more conservative pressure targets, more careful OCT interpretation, and more frequent monitoring than a non-myopic patient with equivalent measured pressures.
Vascular Risk Factors: The Systemic Contributors
Glaucoma, particularly normal tension glaucoma, has a significant vascular component. The optic nerve depends on adequate, well-regulated blood flow. Conditions that impair vascular autoregulation or reduce perfusion contribute to nerve damage independently of intraocular pressure.
Migraine with aura is associated with glaucoma progression. The same cortical spreading depression and vasospasm that produces the migraine aura can affect the posterior ciliary circulation and cause episodic optic nerve ischaemia.
Raynaud’s phenomenon, episodic vasospasm of the extremities, is similarly associated with NTG. The vasospastic tendency that causes cold hands and feet also affects the microvasculature of the optic nerve.
Anaemia reduces oxygen delivery to the optic nerve and can accelerate progression in borderline cases. Obstructive sleep apnoea, covered in detail in a separate article, causes nocturnal hypoxia and IOP spikes that operate entirely outside clinical monitoring.
A complete glaucoma risk assessment includes a systemic vascular history. It is not sufficient to measure eye pressure, examine the disc, and send the patient home. The systemic picture matters.
What This Means for Your Monitoring
Understanding your personal risk profile changes what investigations are appropriate and what targets are realistic.
A patient with thin corneas, a history of disc haemorrhages, nocturnal dipping on antihypertensives, and high myopia has a fundamentally different risk profile from a patient with normal corneas, stable discs, well-controlled blood pressure, and no myopia: even if their measured IOPs are identical.
The first patient needs more aggressive pressure targets, more frequent OCT and field testing, 24-hour IOP monitoring consideration, an ambulatory blood pressure study, and a sleep apnoea screen. The second patient may be safely monitored annually with standard measurements.
If you have glaucoma and have never had a conversation about any of the factors above, you are not receiving complete care. A second opinion that includes a structured risk assessment, not just a pressure check, may change your management in ways that protect your vision for decades.
Clinical Reality (What’s not always obvious)
- Progression in glaucoma is not equal across patients—two people with the same eye pressure can behave very differently over time.
- “Controlled pressure” does not guarantee safety—factors like thin cornea, fragile optic nerve, or vascular instability can drive faster damage.
- Systemic conditions (e.g., obstructive sleep apnea, low blood pressure at night, diabetes) can accelerate progression silently.
- Missed doses, drop intolerance, or poor absorption reduce real-world protection even when prescriptions look adequate.
- Progression is often only obvious in retrospect—which is why early, consistent follow-up matters more than occasional “good” visits.
What You Must Remember
| Factor | What It Means for You |
|---|---|
| Eye pressure level | Higher pressure → higher risk, but not the only driver |
| Optic nerve susceptibility | Some nerves are more vulnerable even at lower pressures |
| Corneal thickness | Thin cornea can underestimate risk and true pressure |
| Type of glaucoma | Normal tension vs high-pressure behave differently |
| Blood flow factors | Poor perfusion or fluctuations affect optic nerve health |
| Systemic conditions | Sleep apnoea, diabetes, vascular disease increase risk |
| Medication adherence | Irregular use reduces protection significantly |
| Response to treatment | Some patients are non-responders to certain drops |
| Stage at diagnosis | Late detection = faster apparent progression |
| Follow-up consistency | Long gaps → missed early warning signs |
| Big picture | Glaucoma progression is multi-factorial—pressure is just one piece of the puzzle |
Frequently Asked Questions
Why is my glaucoma getting worse even though my eye pressure is controlled?
Intraocular pressure is one of several factors driving glaucoma progression. Thin corneas, disc haemorrhages, nocturnal blood pressure dipping, sleep position, myopia, and vascular conditions can all accelerate damage independently of measured IOP. A structured risk assessment should investigate these factors in any patient with unexplained progression.
What is a disc haemorrhage and should I be worried?
A disc haemorrhage is a small bleed at the optic disc margin. It is one of the strongest predictors of glaucoma progression and indicates localised ischaemia at the nerve head. If one is detected, it should prompt a review of pressure targets, vascular risk factors, and monitoring frequency, not simply be noted and observed.
Does blood pressure affect glaucoma?
Yes, significantly. Low blood pressure, particularly nocturnal over-dipping, reduces optic nerve perfusion pressure and accelerates glaucomatous damage. Evening antihypertensive medications can exacerbate nocturnal dipping. A 24-hour ambulatory blood pressure monitor identifies this pattern and can guide medication timing.
Does sleep position affect eye pressure?
Yes. The dependent eye in a side-sleeping patient has measurably higher IOP than the fellow eye, due to increased episcleral venous pressure. In patients with asymmetric glaucoma, sleep position may be a contributing factor. Head-of-bed elevation reduces nocturnal IOP in both eyes.
Does myopia make glaucoma worse?
High myopia makes the optic nerve more vulnerable to glaucomatous damage at any given pressure. The lamina cribrosa in a myopic eye is structurally weaker and deforms at lower pressure thresholds. Myopic patients with glaucoma require more conservative targets and more careful monitoring.
What is central corneal thickness and why does it matter?
Central corneal thickness affects the accuracy of IOP measurement and is an independent risk factor for glaucoma progression. Thin corneas lead to underestimation of true IOP and carry intrinsically higher progression risk. Every glaucoma patient should have their corneal thickness measured and their pressure readings interpreted in that context.
Read the research articles.
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine,.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
More Glaucoma Eye Drops is Not Better Glaucoma Care
More glaucoma eye drops do not guarantee better control. Treatment must be individualised based on risk, progression, and tolerance. Overmedication…