Family History & Glaucoma Screening– My Parent or Sibling Has Glaucoma. Do I Need to Get Tested Too? Short answer, YES. Having a first degree relative with glaucoma: a parent, sibling, or child, raises your lifetime risk of developing the disease by four to nine times compared to someone with no family history, says Dr Shibal Bhartiya.
Your parent or sibling has just been diagnosed with glaucoma. Or perhaps they have had it for years and you are only now realising what that means for you.
You are asking the right question. Most people do not ask it until it is too late. Dr Shibal Bhartiya explains more.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Why Family History Changes Everything in Glaucoma
Glaucoma is not random. It runs in families. Having a first degree relative with glaucoma: a parent, sibling, or child, raises your lifetime risk of developing the disease by four to nine times compared to someone with no family history.
That is not a small increase. That is a fundamental shift in your risk category.
And yet most first degree relatives of glaucoma patients never get tested. They wait for symptoms. Glaucoma does not produce symptoms until significant, often irreversible damage has already occurred. By the time your vision changes, the window for early intervention has often narrowed considerably.
This is why family history glaucoma screening exists: not to frighten you, but to find the disease before it finds you.
What Is the First Degree Relative Glaucoma Risk?
A first degree relative is a parent, sibling, or child: someone who shares approximately 50 percent of your genetic material.
The first degree relative glaucoma risk is well established in research. Studies consistently show that having one affected first degree relative raises your risk of developing primary open angle glaucoma to approximately 1 in 5. Having two affected first degree relatives raises it further.
The risk is highest when the affected relative developed glaucoma before the age of 60, when the disease was severe at diagnosis, or when the relative required surgery rather than drops alone.
First degree relative glaucoma risk is also higher in specific ethnic groups. People of African descent carry a higher baseline risk. In India, primary angle closure glaucoma has a higher prevalence than in Western populations, and this pattern also clusters in families.
Knowing your family history is not just useful. In glaucoma, it is clinically essential.
Does Having a Family History Mean You Will Definitely Get Glaucoma?
No. A family history raises your risk. It does not guarantee disease.
Many people with a strong family history never develop glaucoma. Many develop it only in their seventies or eighties, when treatment is straightforward and vision loss is entirely preventable with monitoring.
What family history means clinically is this: you belong in a higher-risk group that benefits from earlier, more frequent screening for glaucoma. That is all. It is not a sentence. It is a schedule.
Glaucoma Risk Factors Beyond Family History
Family history is the single strongest glaucoma risk factor after age. But it does not act alone. Several other glaucoma risk factors combine with family history to raise your personal risk further.
Age is the most consistent glaucoma risk factor across all populations. Risk rises steeply after 40 and continues to increase with each decade.
Raised eye pressure, also called ocular hypertension, is a major modifiable glaucoma risk factor. Not everyone with high eye pressure develops glaucoma, but the risk is substantially elevated, particularly when combined with family history.
Myopia (near-sightedness) increases glaucoma risk, particularly for primary open angle glaucoma. Moderate to high myopia is an independent glaucoma risk factor.
Thin corneas reduce the accuracy of eye pressure measurements and are independently associated with glaucoma progression risk.
Systemic conditions including diabetes, hypertension, and migraine are associated with higher glaucoma risk in some studies, particularly for normal tension glaucoma.
Previous eye injury or steroid use — whether eye drops, inhalers, skin creams, or oral steroids — can raise eye pressure and trigger steroid-induced glaucoma, particularly in genetically susceptible individuals.
When you combine a family history of glaucoma with one or more of these additional glaucoma risk factors, the case for early screening becomes compelling.
What Does Screening for Glaucoma in Adults Actually Involve?
Screening for glaucoma in adults is not a single test. It is a short, structured examination that covers the four main parameters of glaucoma assessment.
Eye pressure measurement — intraocular pressure is measured using a non-contact tonometer or applanation tonometry. This takes less than a minute. It is painless.
Optic nerve assessment — the ophthalmologist examines the optic disc through a dilated pupil or with specialist lenses. The size, shape, and symmetry of the optic nerve head are evaluated. This is the most important part of any glaucoma screening examination.
Corneal thickness measurement — pachymetry measures corneal thickness, which affects the interpretation of eye pressure readings.
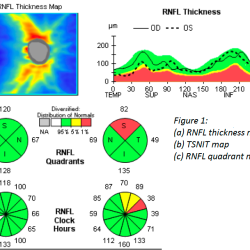
OCT imaging — optical coherence tomography of the RNFL and optic nerve head provides structural data that can detect early glaucoma damage before any symptoms or visual field changes occur. You can read more about what an OCT scan shows and how to interpret your report.
Visual field testing — in higher-risk individuals, a visual field test maps peripheral and central vision to detect any functional loss.
Gonioscopy — in patients where angle closure is suspected, gonioscopy examines the drainage angle of the eye. This is particularly relevant in Indians, where angle closure glaucoma is more prevalent.
A complete screening for glaucoma in adults takes approximately 45 to 60 minutes at a specialist glaucoma clinic, including dilation time.
When Should Screening for Glaucoma Early Begin?
The timing of screening for glaucoma early depends on your personal risk profile.
For most adults with a first degree relative with glaucoma and no other risk factors, screening should begin at 40. Some guidelines recommend starting at 35 in high-risk ethnic groups or when the affected relative had early-onset disease.
For adults with a family history plus additional glaucoma risk factors: high myopia, raised eye pressure found incidentally, or very thin corneas, earlier screening is warranted. In these cases, a baseline examination in the mid-thirties is reasonable.
For adults with no family history and no other risk factors, screening for glaucoma in adults is generally recommended from the age of 40 as part of a routine comprehensive eye examination.
The question is not whether to screen. The question is when to start and how often to repeat.
How Often Should You Be Screened?
Frequency depends on what the first examination shows.
If the first screening is entirely normal: normal eye pressure, healthy optic nerve, normal OCT, annual or biennial review is appropriate for most people in the family history risk group.
If the first screening shows borderline findings: slightly elevated pressure, a suspicious optic disc, or mildly thin RNFL on OCT, more frequent monitoring is needed. Your glaucoma specialist will advise a specific schedule based on your individual findings.
If the first screening confirms early glaucoma, you move from a screening pathway to a treatment and monitoring pathway. Early glaucoma detected through family history glaucoma screening is almost always manageable, and vision loss is highly preventable with timely intervention.
Detecting Glaucoma Early: Why It Matters So Much
Glaucoma destroys retinal nerve fibres. Once those fibres are gone, they do not regenerate. The vision lost to glaucoma does not return.
Detecting glaucoma early changes the entire trajectory of the disease. A patient diagnosed at the very beginning of structural damage, before any visual field loss, has an excellent long-term prognosis with appropriate treatment. A patient diagnosed after significant optic nerve damage faces a harder, narrower path.
The difference between these two patients is often not biology. It is timing. It is whether someone in the family said: you should get checked, and whether the person listened.
Detecting glaucoma early through structured family history screening is one of the highest-value interventions in all of preventive ophthalmology. It costs very little. It changes lives.
What Happens If Glaucoma Is Found?
Finding glaucoma early through family history glaucoma screening is not bad news. It is good news delivered at the right time.
Early glaucoma in a screened patient is almost always managed with eye drops alone. Treatment is started, eye pressure is brought to a safe target, and the optic nerve is monitored regularly. Most patients with early glaucoma, managed well and consistently, never develop significant visual impairment.
The goal of glaucoma treatment is not to cure the disease. It is to slow it so completely that it never affects your quality of life. That goal is realistic. It is achieved every day for patients who are found early.
What changes if glaucoma is found is not your life. It is your schedule, a few extra clinic visits and a bottle of eye drops. That is the trade. For preserved vision over decades, it is a very good trade.
What If the Screening Is Normal?
A normal screening result is genuinely reassuring, but it is not a permanent all-clear.
Glaucoma can develop or progress at any age. A normal result at 40 means you do not have glaucoma now. It does not mean you will never develop it. This is why regular, repeated family history glaucoma screening matters more than a single normal result.
Think of it the way you think of blood pressure checks or dental appointments. A normal result today schedules your next check. It does not cancel all future checks.
Where to Get Screened in Gurgaon
If you have a family history of glaucoma and have not yet been assessed, a structured glaucoma risk evaluation with a glaucoma specialist in Gurgaon is the right next step.
A specialist assessment goes beyond a basic eye pressure check. It includes optic nerve imaging, corneal thickness measurement, OCT analysis, and visual field testing, and if indicated, gonioscopy. This gives you a complete, documented baseline against which future examinations can be compared.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram. She offers structured glaucoma risk assessments for patients with a family history of glaucoma, including those seeking a second opinion on existing results or diagnoses.
Appointments: +91 88826 38735
Upload your reports for a structured review.
Gentle Takeaway
Your parent’s diagnosis is information. It is not fate.
The single most useful thing you can do with that information is act on it early, before symptoms, before damage, before the window narrows.
Glaucoma caught early is a very manageable disease. Glaucoma caught late is a much harder conversation. The difference is often a single timely appointment.
Book one.
Family History as a Glaucoma Risk Trigger, Not a Footnote
A positive family history remains one of the most clinically actionable risk signals in glaucoma, yet also one of the most under-leveraged.
First-degree relatives of patients with glaucoma have a substantially higher lifetime risk (often 3–4× or more), and importantly, may develop disease earlier and with more aggressive trajectories.
Dr Bhartiya’s editorial along with geneticists from AIIMS, New Delhi and Marengo Asia, emphasises on integrating genomics into practice (PMID: 41523176), reinforcing that family history is not merely a background detail but a proxy for inherited susceptibility that should actively trigger structured screening pathways.
In practical terms, this shifts glaucoma care from opportunistic detection to targeted risk-based screening, where identifying and counselling family members becomes a core extension of clinical responsibility, not an optional add-on.
Clinical Reality (Family History & Glaucoma Screening in India)
- Family history is one of the strongest risk factors — but often ignored
Many patients only realise its importance after damage has already occurred. - Screening is not routine for relatives
Unlike diabetes or hypertension, glaucoma screening is rarely proactively advised to family members. - “No symptoms” delays first check
High-risk individuals often wait for visual complaints, by which time disease may already be advanced. - Normal eye check-ups may miss early glaucoma
Routine vision tests without optic nerve evaluation or fields can miss disease. - Younger family members are often overlooked
Screening is delayed until later decades, despite risk beginning earlier. - One normal test gives false reassurance
A single normal OCT or pressure reading does not rule out future risk.
What Good Screening Looks Like (If You Have a Family History of Glaucoma)
- Early baseline screening — before symptoms
Ideally by age 30–40, or earlier if multiple affected relatives. - Comprehensive evaluation, not just vision or pressure
Includes optic nerve assessment, OCT, visual fields, corneal thickness. - Risk-stratified follow-up
Frequency depends on baseline findings — not “come if needed.” - Family-based screening approach
First-degree relatives (parents, siblings, children) are actively advised evaluation. - Longitudinal monitoring
Tracking change over time is key — not single reports. - Clear patient education
Understanding risk improves adherence to follow-up and screening.
Family History & Glaucoma Screening: What’s Missed vs What Matters
| Situation | What Patients Often Assume | Clinical Reality (India Context) | What Good Care Looks Like |
|---|---|---|---|
| Family history present | “It’s not affecting me yet” | Risk is significantly higher even without symptoms | Early baseline screening for all first-degree relatives |
| No symptoms | “I’ll get checked if I notice a problem” | Glaucoma remains silent until irreversible damage | Screening before symptoms begin |
| Routine eye check-up | “My eyes were checked, so I’m fine” | Standard vision tests may miss early glaucoma | Comprehensive glaucoma evaluation (OCT + fields + nerve exam) |
| Age factor | “I’m too young to worry” | Risk can begin earlier in those with family history | Screening from 30–40 years or earlier if high risk |
| Single normal report | “Everything was normal last time” | One test cannot rule out future progression | Periodic follow-up based on risk profile |
| Family awareness | “No one told my family to get tested” | Screening advice is often not extended to relatives | Proactive, family-based screening approach |
| Follow-up | “I’ll come back if needed” | Irregular follow-up delays detection of early changes | Structured, risk-based follow-up intervals |
| Understanding risk | “It’s just genetic, nothing to do now” | Early detection can prevent vision loss | Education + long-term monitoring strategy |
| Disease perception | “Glaucoma means high pressure only” | Many patients develop glaucoma at normal pressures | Broader risk assessment beyond IOP |
| Goal of screening | “Just to rule it out” | Screening is about early detection and tracking change | Long-term risk management, not one-time clearance |
Frequently Asked Questions: Family History and Glaucoma Screening
Does glaucoma run in families?
Yes. Having a first degree relative: a parent, sibling, or child with glaucoma raises your lifetime risk of developing the disease by four to nine times. Family history is the single strongest glaucoma risk factor after age. Structured family history glaucoma screening is recommended for all first degree relatives of glaucoma patients.
What is the risk of glaucoma if a parent has it?
The first degree relative glaucoma risk is approximately 1 in 5 for primary open angle glaucoma, significantly higher than the general population risk of around 1 in 50. The risk is higher when the affected parent developed glaucoma early, had severe disease, or required surgery.
At what age should I get screened for glaucoma if a parent has it?
Screening for glaucoma early should begin at 40 for most adults with a first degree relative with glaucoma. Those with additional glaucoma risk factors, high myopia, raised eye pressure, or thin corneas, should consider a baseline examination from the mid-thirties.
What does glaucoma screening involve?
Screening for glaucoma in adults includes eye pressure measurement, optic nerve assessment through a dilated pupil, corneal thickness measurement, OCT imaging of the nerve fibre layer, and visual field testing in higher-risk individuals. A complete specialist assessment takes approximately 45 to 60 minutes.
Can glaucoma skip a generation?
Yes. The genetic inheritance pattern of glaucoma is complex and not fully understood. Glaucoma can skip generations or manifest differently across family members. A negative family history in your parents does not fully exclude risk if grandparents or siblings are affected.
What glaucoma risk factors increase my risk beyond family history?
Key glaucoma risk factors that combine with family history include age over 40, raised eye pressure, moderate to high myopia, thin corneas, diabetes, and previous steroid use. The more risk factors present alongside family history, the stronger the case for early and frequent screening.
If my glaucoma screening is normal, do I still need follow-up?
Yes. A normal result at first screening does not mean permanent all-clear. Glaucoma can develop at any point. Annual or biennial review is recommended for adults with a family history of glaucoma, even when the initial assessment is entirely normal.
Book a consultation with Dr Shibal Bhartiya:
Marengo Asia Hospitals, Gurugram
Phone: +91 88826 38735
Website: drshibalbhartiya.com
Google Business Profile: maps.app.goo.gl/mcfegmHTuhqV5hSp6
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma