Early detection. Risk-based care. Long-term vision protection. Glaucoma often develops silently, but the risk can be identified early with the…
Tag: Dr Shibal Bhartiya glaucoma care Gurgaon
Glaucoma Care in Gurgaon
Dr Shibal Bhartiya provides glaucoma care in Gurgaon, focusing on early detection, risk stratification, and long-term management of glaucoma to prevent irreversible vision loss. Care typically includes detailed optic nerve evaluation, OCT and visual fields, and personalised treatment plans tailored to disease stage and progression risk.
Early detection. Risk-based care. Long-term vision protection. Glaucoma often develops silently, but the risk can be identified early with the right tests and careful interpretation, before vision loss becomes irreversible. Dr Shibal Bhartiya, fellowship-trained glaucoma specialist in Gurgaon, brings together evidence-based insights on screening, risk stratification, and long-term care to help protect vision over time.
Glaucoma is a silent, progressive disease. Vision loss often occurs gradually and cannot be reversed. The goal of care is not just lowering eye pressure, but protecting the optic nerve safely over time.
If you are looking for a glaucoma specialist in Gurgaon, treatment decisions should be based on risk, progression, and long-term safety, not just the number of medications.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
🧠 A Different Approach to Glaucoma Care
Glaucoma is often managed reactively, pressure rises, more drops are added. But glaucoma is a long-arc disease.
Effective care focuses on:
- Early detection before irreversible damage
- Risk stratification, not one-size-fits-all treatment
- Judicious use of medications
- Minimising side effects and treatment burden
- Long-term stability, not short-term numbers
This is not about doing more. It is about doing what is right, at the right time.
🔎 Start Here: Understanding Your Glaucoma
If you are trying to understand your diagnosis or treatment, these guides will help:
- Learn why more glaucoma eye drops are not always better and when simplifying treatment may be safer
→ https://drshibalbhartiya.com/more-glaucoma-eye-drops-not-better-care/ - Understand when to seek a glaucoma second opinion if your treatment feels unclear or complex
→ https://drshibalbhartiya.com/glaucoma-second-opinion-gurgaon/ - Recognise the early symptoms of glaucoma people often miss
→ https://drshibalbhartiya.com/glaucoma-early-symptoms/ - See how family history increases glaucoma risk and why screening matters
→ https://drshibalbhartiya.com/family-history-glaucoma-screening/ - Understand how OCT and visual fields track glaucoma progression over time
→ https://drshibalbhartiya.com/oct-visual-field-interpretation/
⚠️ When Should You Be Concerned?
You should consider evaluation if you have:
- Family history of glaucoma
- Increasing number of eye drops
- Redness, irritation, or intolerance to medications
- “Normal” eye pressure but worsening reports
- Difficulty understanding your treatment plan
Glaucoma often progresses silently. Waiting for symptoms can delay care.
If this sounds familiar, it may be time to consider a glaucoma second opinion:
https://drshibalbhartiya.com/glaucoma-second-opinion-gurgaon/
🧪 How Glaucoma Is Evaluated
Accurate glaucoma care requires more than a pressure check.
Assessment includes:
- Optic nerve evaluation
- OCT (optic nerve imaging)
- Visual field testing
- Corneal thickness
- Risk profiling over time
Understanding glaucoma progression through OCT and visual field analysis is key to making safe treatment decisions.
💊 Treatment Is Not Just About Eye Drops
Treatment options may include:
Adding more medications is not always the safest approach.
In many cases, treatment strategy matters more than the number of drops used:
https://drshibalbhartiya.com/more-glaucoma-eye-drops-not-better-care/
Managing side effects of glaucoma drops
🔁 Long-Term Care Matters
Glaucoma requires:
- Regular follow-up
- Consistent monitoring
- Adjustment based on progression
The goal is:
- Stable vision
- Minimal side effects
- Sustainable treatment
👁️ Not Sure Where You Stand?
If:
- you are on multiple eye drops
- your reports are difficult to interpret
- or your condition seems to be progressing
A structured evaluation can help simplify your treatment.
👉 Request a glaucoma second opinion:
https://drshibalbhartiya.com/glaucoma-second-opinion-gurgaon/
Clinical Reality (What’s not always obvious)
- Good glaucoma care is not a one-time consultation—it’s longitudinal monitoring of glaucoma over years.
- A “normal” eye pressure does not guarantee safety—progression can occur despite seemingly controlled numbers.
- Technology (OCT, visual fields) supports care, but clinical judgement and pattern recognition over time are what prevent vision loss.
- Over-treatment (too many drops) and under-treatment (delayed escalation) are both risks—balance is key.
- The quality of follow-up and consistency of care often matter more than any single test or visit.
What you Must Remember
| Aspect | What It Means for You |
|---|---|
| Core goal | Preserve vision long-term by slowing disease progression |
| Key evaluations | Optic nerve exam, OCT, visual fields, eye pressure |
| Treatment options | Eye drops, laser (SLT), surgery if needed |
| Follow-up importance | Regular monitoring detects early progression |
| Personalisation | Care tailored to risk, lifestyle, and response |
| When to seek specialist care | Uncertain diagnosis, progression, second opinion |
| Role of technology | Supports early detection and tracking |
| Systemic factors | Sleep, blood pressure, health influence outcomes |
| Patient role | Adherence to treatment and follow-up is critical |
| Big picture | Glaucoma care is ongoing risk management, not a one-time fix |
FAQs About Glaucoma Care in Gurgaon
When should I see a glaucoma specialist in Gurgaon?
You should see a glaucoma specialist if you have a family history of glaucoma, are on an increasing number of eye drops, experience redness or irritation from your medications, have been told your eye pressure is normal but your reports are worsening, or find your current treatment plan difficult to understand. Glaucoma often progresses silently. Waiting for symptoms can delay care and lead to irreversible vision loss.
What tests are done in a glaucoma evaluation?
A comprehensive glaucoma evaluation includes optic nerve examination, OCT imaging of the optic nerve and retinal nerve fibre layer, visual field testing, corneal thickness measurement, and risk profiling over time. A pressure check alone is not sufficient to evaluate or manage glaucoma safely. Each of these tests contributes a different piece of information about disease risk and progression.
What is a glaucoma second opinion and when is it needed?
A glaucoma second opinion is a structured, independent review of your diagnosis and treatment plan. It is useful when you are on multiple eye drops, when your condition seems to be progressing despite treatment, when reports are difficult to interpret, or when your treatment plan feels unclear. Dr Shibal Bhartiya offers dedicated glaucoma second opinion consultations in Gurgaon, with a focus on simplifying decisions and protecting vision long-term.
Is adding more eye drops always the right treatment for glaucoma?
No. Adding more medications is not always the safest or most effective approach. Glaucoma treatment should be based on risk, rate of progression, side effect burden, and long-term safety. In many cases, treatment strategy matters more than the number of drops prescribed. Laser procedures or surgical options may be more appropriate than escalating medications, depending on the individual case.
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma
Related Reading
Get an Online Glaucoma Consult
Why Do I Need a Visual Field Test?
Understanding Your OCT Report in Glaucoma
Visual Field and OCT: Structure & Function Correlation
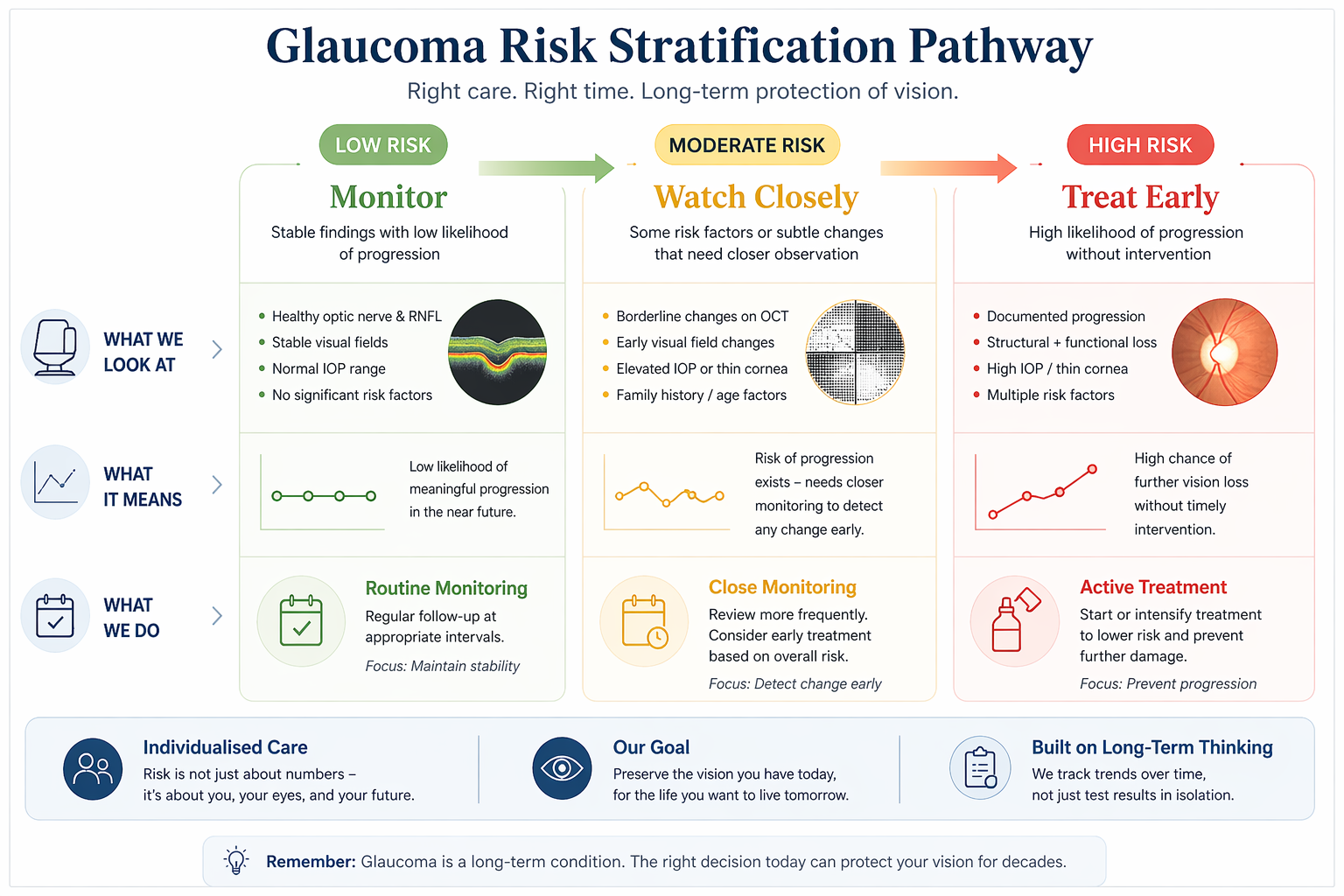
Risk Stratification in Glaucoma
Risk stratification in glaucoma means assessing how likely the disease is to progress and how aggressively it should be treated. It combines optic nerve findings, eye pressure, test results, and systemic factors to guide personalised, long-term care, explains Dr Shibal Bhartiya.
Most glaucoma decisions are not about what your reports show today. They are about what your eyes are likely to do over the next 5–10 years.
Risk stratification in glaucoma helps decide who needs treatment, who can be safely monitored, and who may be at risk of silent progression, even when tests appear normal. Dr Bhartiya explains.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
🧩 WHAT THIS REALLY MEANS

Why glaucoma care is not one-size-fits-all
Two patients can have similar reports, and very different futures.
- One may remain stable for years
- Another may lose vision slowly without obvious warning
Risk stratification is the process of identifying this difference early. It helps answer the most important question:
👉 What is likely to happen if we do nothing?
⚠️WHAT MOST PEOPLE GET WRONG
Why reports alone don’t tell the full story
Many glaucoma decisions are based only on:
These are important, but incomplete.
Because:
- Structural damage can begin before symptoms
- Functional loss appears late
- Test results can fluctuate
- “Normal” does not always mean “safe”
👉 This is where many patients are either over-treated unnecessarily, or under-treated until it’s too late
🧠 HOW RISK IS ACTUALLY ASSESSED
What we look at beyond individual test results.
Risk stratification considers patterns over time, not isolated numbers.
1. Structural changes
Subtle optic nerve or OCT changes that may precede symptoms
2. Functional trends
Visual field patterns, even when still within “normal” range
3. Rate of change
How quickly (or slowly) things are evolving
4. Individual risk factors
- Family history
- Age
- Corneal thickness
- Baseline nerve health
5. Life context
How much vision loss would affect your daily function
👉 This is not just diagnosis. It is future risk prediction.
Dr Bhartiya, along with her associates, write about the current perspectives in tackling glaucoma blindness. These include raising awareness, enhancing early detection programs, and access to care, particularly in underserved populations. Pubmed.
🔍 THREE COMMON SCENARIOS
When we treat, when we monitor, and when we watch closely
🟢 Low risk
- Stable findings
- No clear progression
👉 Safe to monitor with regular follow-up
🟡 Moderate risk
- Suspicious changes
- Uncertain progression
👉 Close monitoring or early treatment depending on context
🔴 High risk
- Clear progression
- Structural + functional change
👉 Treatment is recommended to prevent further loss
👉 The goal is not to treat everyone. The goal is to treat the right patients at the right time.
⏳ THE LONG-ARC VIEW
Why early clarity matters more than late intervention
Glaucoma does not usually cause sudden symptoms. It progresses quietly. Patients may feel:
- Slight reading difficulty
- Reduced contrast
- Night discomfort
- Slower visual processing
By the time vision feels obviously affected, damage is often already established.
👉 Risk stratification in glaucoma allows intervention before this stage.
What You Must Remember
| Component | What It Means for You |
|---|---|
| Optic nerve status | Structural damage and vulnerability define baseline risk |
| Eye pressure (IOP) | Important driver, but must be interpreted in context |
| OCT findings | Early structural loss may signal higher future risk |
| Visual fields | Functional impact and progression tracking |
| Corneal thickness | Influences true pressure interpretation and risk |
| Type of glaucoma | Normal tension vs high-pressure behave differently |
| Systemic factors | Sleep apnoea, BP fluctuations, diabetes affect progression |
| Rate of change | Faster progression = higher risk category |
| Adherence to treatment | Inconsistent use increases real-world risk |
| Follow-up pattern | Regular monitoring allows timely risk recalibration |
| Big picture | Risk stratification guides target pressure, treatment intensity, and follow-up frequency |
Clinical Reality (What’s not always obvious)
Risk stratification is not about labels—it’s about deciding how closely to monitor and how aggressively to treat over time.
Risk in glaucoma is dynamic, not fixed—it changes with time, response to treatment, and systemic health.
The same eye pressure can be “safe” for one patient and damaging for another depending on optic nerve susceptibility.
Test results don’t always align—OCT, fields, and clinical exam may show different pieces of the puzzle.
Systemic factors (blood pressure dips, vascular instability, obstructive sleep apnea) can silently shift risk.
🧍♀️WHY SECOND OPINIONS MATTER HERE
When it’s worth taking a step back
You may benefit from a second opinion if:
- You’ve been advised long-term treatment without clarity
- You’ve been told to “just monitor” without explanation
- Your reports seem normal, but symptoms persist
- Your treatment keeps changing
Sometimes, the issue is not the test. It is the interpretation.
🚨 Need clarity about your glaucoma risk?
You don’t need more reports. You need to understand what they mean over time.
👉 Request a Second Opinion Consultation
Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides trusted second opinions for patients seeking clarity before major treatment decisions. Both, in person, and online.
🔎 Frequently Asked Questions
What is risk stratification in glaucoma?
It is the process of assessing how likely glaucoma is to progress over time, based on multiple factors, not just current test results.
Can glaucoma be present even if tests are normal?
Yes. Early glaucoma may not show clear changes on routine tests, especially in the initial stages.
Does everyone with glaucoma need treatment?
No. Some patients can be safely monitored, while others need early intervention depending on their risk profile.
How often should glaucoma be monitored?
This depends on individual risk. Some patients need frequent follow-up, while others can be reviewed less often.
Why do different doctors give different advice?
Because glaucoma management involves judgement, not just reports. Different interpretations of risk can lead to different recommendations.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma
Why Glaucoma Gets Worse Faster in Some People Than Others
Glaucoma can worsen faster in some people due to differences in optic nerve vulnerability, blood flow, and systemic risk factors, not just eye pressure. Even with “controlled” pressure, glaucoma may progress if underlying risks are not identified and monitored over time, Dr Shibal Bhartiya explains.
Two patients. Same diagnosis. Similar eye pressure. Same drops. One is stable at ten years. The other has lost significant field within three. Patients often ask: Why Glaucoma Gets Worse Faster in Some People Than Others.
This is not unusual in glaucoma. It is one of the most clinically important, and least explained, aspects of the disease. Your doctor told you, you have glaucoma, gave you drops. Called you back for monitoring.
But did you discuss if your optic nerve might be more vulnerable than average? Or, what factors beyond eye pressure are quietly accelerating the damage.
This article, written by Dr Bhartiya, explains those factors. Understanding them changes how glaucoma is monitored, what investigations are relevant, and what questions to ask at your next appointment.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Why Intraocular Pressure Is Only Part of the Story
The historical model of glaucoma was simple: raised intraocular pressure damages the optic nerve. Lower the pressure, stop the damage. This model is incomplete.
Intraocular pressure is the only modifiable risk factor with proven treatment benefit. It remains central to glaucoma management. But a substantial proportion of glaucoma patients, particularly those with normal tension glaucoma, progress despite pressure that is well controlled by any standard definition. And among patients with elevated pressure, some progress quickly while others with similar pressures remain stable for decades.
Pressure level explains some of the variation. The factors below explain the rest.
Central Corneal Thickness: The Hidden Pressure Modifier
Central corneal thickness (CCT) is one of the most important risk factors for glaucoma progression, and one of the most underappreciated by patients.
Intraocular pressure is measured by the resistance the cornea offers to an applanation probe or air puff. A thicker cornea gives artificially high readings. A thinner cornea gives artificially low ones. Standard Goldmann tonometry assumes a corneal thickness of approximately 545 microns. Patients with thinner corneas have their true pressure systematically underestimated at every clinic visit.
But CCT is not merely a measurement correction factor. Thin central cornea is an independent risk factor for glaucoma progression, separate from any pressure effect. The Ocular Hypertension Treatment Study (OHTS) identified CCT below 555 microns as one of the strongest predictors of conversion from ocular hypertension to glaucoma. Patients with thin corneas progress faster and reach endpoints earlier than those with normal or thick corneas, even after adjusting for measured IOP.
If you have glaucoma and have never had your corneal thickness measured, ask for it. It changes how your pressure readings should be interpreted, and it tells your specialist something important about your intrinsic risk.
Disc Haemorrhages: The Warning Signal That Gets Missed
A disc haemorrhage is a small, splinter-shaped bleed at the margin of the optic disc. It is visible on fundus examination and resolves within weeks to months. Most patients never know they have had one.
Disc haemorrhages are one of the strongest predictors of glaucoma progression. They indicate localised ischaemia, a transient interruption of blood flow, at the optic nerve head, and they mark the site of imminent or ongoing retinal nerve fibre layer loss. Studies consistently show that the sector of the optic nerve that bleeds is the sector that subsequently loses nerve fibres on OCT, and the sector where visual field loss subsequently develops.
In normal tension glaucoma, disc haemorrhages are particularly common and particularly significant. Their presence in an NTG patient is a direct signal that vascular insufficiency is active and that the nerve is under ischaemic stress beyond whatever pressure-related stress is present.
A patient whose disc haemorrhage is detected at a routine visit is not unlucky. The hemorrahe is a timely warning. The appropriate response is not to note it and move on. It is to ask why the bleed occurred, whether pressure targets need revision, and whether vascular risk factors need investigation.
Systemic Hypotension and Nocturnal Dipping
The optic nerve is supplied by blood from the posterior ciliary arteries. Like all tissues, it requires adequate perfusion pressure, the difference between arterial blood pressure and intraocular pressure, to receive oxygen and nutrients. When perfusion pressure falls, optic nerve gets less blood supply.
Systemic hypotension is a direct cause of reduced optic nerve perfusion pressure. It is most relevant at night. During sleep, blood pressure falls physiologically, this is normal nocturnal dipping. In some people, blood pressure dips excessively, by more than 20 percent from daytime levels. This is called nocturnal over-dipping.
Nocturnal over-dipping is strongly associated with glaucoma progression, particularly in normal tension glaucoma. The optic nerve, already under whatever pressure stress is present, faces additional ischaemic stress during the hours of maximum blood pressure reduction, precisely when patients are asleep and not being monitored.
The clinical implications are significant. Antihypertensive medications taken in the evening can exacerbate nocturnal dipping. A glaucoma patient who begins a new blood pressure medication and subsequently shows accelerated progression deserves a medication timing review. Taking antihypertensives in the morning rather than the evening, where clinically possible, may reduce nocturnal dipping and its consequences for the optic nerve.
A 24-hour ambulatory blood pressure monitor is a simple, non-invasive investigation that identifies nocturnal dipping. In standard glaucoma management, doctors forget about night time BP. In any patient with normal tension glaucoma or unexplained progression, however, it is essential.
Sleep Position: The Factor Nobody Mentions
The side on which a patient sleeps affects their intraocular pressure. This is documented, reproducible, and almost never discussed.
IOP is higher in the dependent eye, the eye facing down, when lying on one side. The mechanism involves increased episcleral venous pressure from the gravitational position. For a patient who sleeps consistently on one side, the dependent eye is exposed to elevated pressure for six to eight hours every night. Entirely outside the window of clinic measurement.
Studies using continuous IOP monitoring have shown that the dependent eye IOP during sleep can be 3 to 6 mmHg higher than the fellow eye. This is a clinically significant asymmetry in a disease. Especially where even 1 mmHg differences in pressure can result in measurable differences in progression rates.
This is relevant for any patient with asymmetric glaucoma, where one eye is worse than the other despite similar measured IOPs. If the worse eye is consistently the dependent eye, sleep position may be contributing.
Head-of-bed elevation, raising the head of the bed by 20 to 30 degrees, may reduce nocturnal IOP in both eyes. It is a simple, free, non-pharmacological intervention with evidence behind it.
Myopia: The Optic Nerve That Was Already Vulnerable
High myopia, short-sightedness above minus 3 to 5 dioptres, is an independent risk factor for glaucoma and for faster progression. The mechanism involves the structural anatomy of the myopic eye.
In a myopic eye, the scleral canal through which the optic nerve exits, the lamina cribrosa, is tilted, stretched, and biomechanically weaker than in an emmetropic eye. This altered geometry means the optic nerve is more susceptible to the same level of intraocular pressure that a normal eye would tolerate well. The lamina cribrosa in a myopic eye bends and deforms at lower pressure thresholds.
Myopic eyes also have thinner retinal nerve fibre layers at baseline: not from glaucoma, but from the axial elongation that stretches the retina. This makes OCT interpretation more complex: the baseline is lower, so the threshold for detecting abnormality shifts, and early glaucomatous loss can be masked within the range of normal myopic variation.
A highly myopic patient with glaucoma requires more conservative pressure targets, more careful OCT interpretation, and more frequent monitoring than a non-myopic patient with equivalent measured pressures.
Vascular Risk Factors: The Systemic Contributors
Glaucoma, particularly normal tension glaucoma, has a significant vascular component. The optic nerve depends on adequate, well-regulated blood flow. Conditions that impair vascular autoregulation or reduce perfusion contribute to nerve damage independently of intraocular pressure.
Migraine with aura is associated with glaucoma progression. The same cortical spreading depression and vasospasm that produces the migraine aura can affect the posterior ciliary circulation and cause episodic optic nerve ischaemia.
Raynaud’s phenomenon, episodic vasospasm of the extremities, is similarly associated with NTG. The vasospastic tendency that causes cold hands and feet also affects the microvasculature of the optic nerve.
Anaemia reduces oxygen delivery to the optic nerve and can accelerate progression in borderline cases. Obstructive sleep apnoea, covered in detail in a separate article, causes nocturnal hypoxia and IOP spikes that operate entirely outside clinical monitoring.
A complete glaucoma risk assessment includes a systemic vascular history. It is not sufficient to measure eye pressure, examine the disc, and send the patient home. The systemic picture matters.
What This Means for Your Monitoring
Understanding your personal risk profile changes what investigations are appropriate and what targets are realistic.
A patient with thin corneas, a history of disc haemorrhages, nocturnal dipping on antihypertensives, and high myopia has a fundamentally different risk profile from a patient with normal corneas, stable discs, well-controlled blood pressure, and no myopia: even if their measured IOPs are identical.
The first patient needs more aggressive pressure targets, more frequent OCT and field testing, 24-hour IOP monitoring consideration, an ambulatory blood pressure study, and a sleep apnoea screen. The second patient may be safely monitored annually with standard measurements.
If you have glaucoma and have never had a conversation about any of the factors above, you are not receiving complete care. A second opinion that includes a structured risk assessment, not just a pressure check, may change your management in ways that protect your vision for decades.
Clinical Reality (What’s not always obvious)
- Progression in glaucoma is not equal across patients—two people with the same eye pressure can behave very differently over time.
- “Controlled pressure” does not guarantee safety—factors like thin cornea, fragile optic nerve, or vascular instability can drive faster damage.
- Systemic conditions (e.g., obstructive sleep apnea, low blood pressure at night, diabetes) can accelerate progression silently.
- Missed doses, drop intolerance, or poor absorption reduce real-world protection even when prescriptions look adequate.
- Progression is often only obvious in retrospect—which is why early, consistent follow-up matters more than occasional “good” visits.
What You Must Remember
| Factor | What It Means for You |
|---|---|
| Eye pressure level | Higher pressure → higher risk, but not the only driver |
| Optic nerve susceptibility | Some nerves are more vulnerable even at lower pressures |
| Corneal thickness | Thin cornea can underestimate risk and true pressure |
| Type of glaucoma | Normal tension vs high-pressure behave differently |
| Blood flow factors | Poor perfusion or fluctuations affect optic nerve health |
| Systemic conditions | Sleep apnoea, diabetes, vascular disease increase risk |
| Medication adherence | Irregular use reduces protection significantly |
| Response to treatment | Some patients are non-responders to certain drops |
| Stage at diagnosis | Late detection = faster apparent progression |
| Follow-up consistency | Long gaps → missed early warning signs |
| Big picture | Glaucoma progression is multi-factorial—pressure is just one piece of the puzzle |
Frequently Asked Questions
Why is my glaucoma getting worse even though my eye pressure is controlled?
Intraocular pressure is one of several factors driving glaucoma progression. Thin corneas, disc haemorrhages, nocturnal blood pressure dipping, sleep position, myopia, and vascular conditions can all accelerate damage independently of measured IOP. A structured risk assessment should investigate these factors in any patient with unexplained progression.
What is a disc haemorrhage and should I be worried?
A disc haemorrhage is a small bleed at the optic disc margin. It is one of the strongest predictors of glaucoma progression and indicates localised ischaemia at the nerve head. If one is detected, it should prompt a review of pressure targets, vascular risk factors, and monitoring frequency, not simply be noted and observed.
Does blood pressure affect glaucoma?
Yes, significantly. Low blood pressure, particularly nocturnal over-dipping, reduces optic nerve perfusion pressure and accelerates glaucomatous damage. Evening antihypertensive medications can exacerbate nocturnal dipping. A 24-hour ambulatory blood pressure monitor identifies this pattern and can guide medication timing.
Does sleep position affect eye pressure?
Yes. The dependent eye in a side-sleeping patient has measurably higher IOP than the fellow eye, due to increased episcleral venous pressure. In patients with asymmetric glaucoma, sleep position may be a contributing factor. Head-of-bed elevation reduces nocturnal IOP in both eyes.
Does myopia make glaucoma worse?
High myopia makes the optic nerve more vulnerable to glaucomatous damage at any given pressure. The lamina cribrosa in a myopic eye is structurally weaker and deforms at lower pressure thresholds. Myopic patients with glaucoma require more conservative targets and more careful monitoring.
What is central corneal thickness and why does it matter?
Central corneal thickness affects the accuracy of IOP measurement and is an independent risk factor for glaucoma progression. Thin corneas lead to underestimation of true IOP and carry intrinsically higher progression risk. Every glaucoma patient should have their corneal thickness measured and their pressure readings interpreted in that context.
Read the research articles.
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine,.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Prostaglandin Eye Drops for Glaucoma
Prostaglandin eye drops are first-line treatment for glaucoma, helping lower eye pressure by increasing fluid outflow from the eye. They are usually taken once daily, are highly effective, and play a key role in slowing disease progression when used consistently, Dr Shibal Bhartiya explains.
Glaucoma is called the silent thief of sight for a reason. It rarely hurts. The vision loss it causes: slow, peripheral, irreversible, is not something you feel until it is far advanced. This silence is exactly what makes the most common patient mistake so dangerous: stopping prostaglandin eye drops because you feel fine.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides trusted second opinions for patients seeking clarity before major treatment decisions.
What Are Prostaglandin Analogues?
Prostaglandin analogues are the most widely prescribed first-line drops for glaucoma and ocular hypertension. The family includes latanoprost, bimatoprost, travoprost, and tafluprost. One drop, once a day, usually at night, and the intraocular pressure (IOP) comes down by 25 to 35 percent in most patients.
They work by increasing the outflow of aqueous humour through a pathway called the uveoscleral route, essentially opening a drainage channel that bypasses the conventional meshwork. The pressure falls, the optic nerve is protected, and vision is preserved. This mechanism makes them uniquely effective, and uniquely dependent on consistent daily use.
They do not cure glaucoma. They control it. The moment you stop, the protection stops with them.
The Washout Problem: What Happens When You Stop
The term “washout” comes from clinical research. When scientists design drug trials, they ask patients to stop their current drops for a set period before the study begins, so the drug clears the eye and baseline measurements are accurate. This washout period for prostaglandins is typically four to eight weeks.
What researchers noticed, repeatedly, was that IOP did not simply return to its pre-treatment level during washout. In many patients, it climbed significantly higher. This is the rebound spike. It is not a curiosity. It is a clinical hazard, perhaps mediated by receptor upregulation.
This is not theoretical. Research on intraocular pressure dynamics confirms that pressure fluctuation, not just mean pressure, is an independent risk factor for glaucoma progression. A sharp peak does damage that weeks of good control cannot undo. My own published work examining IOP behaviour and treatment targets reinforces why pressure stability matters as much as the average reading. (Bhartiya et al., PMID 25081325)
The Generic Question: Are All Prostaglandins Equal?
In India, the number of generic travoprost and latanoprost formulations available at any pharmacy is bewildering. Patients are switched between brands by chemists, or offered cheaper alternatives by well-meaning family members. The assumption is that the active molecule is the same, so the drops must be identical.
The evidence complicates that assumption.
Research published in the Journal of Current Glaucoma Practice, directly examined the physical properties of branded versus generic travoprost formulations available in the Indian market. The findings were striking: significant variation in drug concentration, osmolality, pH, and drop volume across different generic products, with some formulations falling outside accepted limits. (Wadhwani, Bhartiya et al., PMID 27536047)
A subsequent review I co-authored examined this question more broadly: the debate about branded versus generic glaucoma drugs is not merely academic. For a chronic, largely asymptomatic disease where adherence is already fragile and the consequences of under-treatment are invisible until serious, the choice of formulation matters. Cost matters too, glaucoma is often a lifelong condition, and expense is a real compliance barrier. But cost savings that come with inconsistent drug delivery are not savings at all. (Bhartiya and Dhingra, PMID 33367157)
The practical message: if your chemist substitutes your glaucoma drop with a different brand, tell your glaucoma specialist. Do not assume equivalence. Do not stop the drops while you investigate.
Why Patients Stop, and What Actually Happens
The most common reasons I hear for stopping prostaglandin drops:
“My eyes looked red, so I stopped.“ Conjunctival redness and a mild burning sensation are common early side effects that usually settle within the first few weeks. Stopping the drops removes the side effect and removes the protection. The right response is to speak to your specialist, not to self-discontinue.
“I felt fine.” Glaucoma is asymptomatic. Feeling fine means nothing about your IOP or your optic nerve. By the time you feel something is wrong with your vision, damage has already happened, and it is permanent.
“I ran out and the chemist didn’t have the same brand.” Running out of drops is the single most common cause of medication gaps. It is also entirely preventable. Treat your glaucoma drops the way you would treat insulin: not as something optional when the bottle runs out.
“My eye pressure was normal at my last visit, so I thought I could stop.” This is perhaps the most understandable mistake, and the most dangerous one. The pressure was normal because the drops were working. Stop the drops, and the pressure rises again, sometimes dramatically. Normal pressure on medication is the goal of treatment, not evidence that treatment is no longer needed.
What Happens During Surgery or Procedures?
There is one medically valid reason to pause prostaglandin drops: when your ophthalmic surgeon specifically instructs you to do so before a procedure. Prostaglandins can affect intraoperative results in certain situations, and the decision to pause them must come from your treating doctor, with a clear plan for the period of interruption.
Even then, the pause is carefully managed. Patients undergoing minimally invasive glaucoma surgery (MIGS) or trabeculectomy are monitored closely during any washout period precisely because of the pressure instability it can cause. The surgical approach for individual patients, including whether and how drops are adjusted, requires the kind of nuanced, personalised judgement that cannot be reduced to a general rule. (Bhartiya et al., PMID 31915728)
If you are not being prepared for surgery, there is no reason to stop your drops. None. Unless asked by your glaucoma specialist.
Side Effects: The Ones Worth Knowing About
Prostaglandin analogues are well tolerated by most patients. But there are a handful of side effects worth discussing with your specialist, not because they should prompt you to stop the drops unilaterally, but because knowing about them means you can manage them properly.
Periorbital changes. Long-term use can cause deepening of the upper eyelid sulcus, mild ptosis, and orbital fat atrophy. These changes are collectively described as prostaglandin-associated periorbitopathy. These are more common with higher-concentration formulations and more likely with bimatoprost than with latanoprost or travoprost. They are not medically dangerous, but they are worth discussing if you notice changes in your appearance.
Iris pigmentation. In patients with mixed-colour irises (hazel, green-brown), prostaglandins can gradually increase melanin in the iris stroma, causing a permanent darkening. This change is irreversible but not harmful to vision.
Eyelash changes. Lengthening, thickening, and increased pigmentation of the eyelashes are a well-known effect. For some patients, this is a welcome side effect. For others, misdirected eyelash growth can cause irritation.
Cystoid macular oedema. Rare, but worth knowing. Patients who have had cataract surgery or uveitis have a slightly higher risk. Any new blurring of central vision in a patient using prostaglandins warrants prompt review.
All of these are manageable. None of them are reasons to stop drops without talking to your specialist first.
The Generic Formulation Trap
I want to return to the question of generics, because it is particularly relevant in the Indian context.
A patient prescribed latanoprost 0.005% may be dispensed any one of a dozen formulations depending on what the pharmacy stocks that day. Most patients have no way of knowing whether the bottle they are using is the same drug at the same effective concentration as what they were prescribed.
The research is clear that not all generic formulations are equal in their physical properties, and that quality control in the production of generic ophthalmic formulations in India has historically been variable. This does not mean all generics are inferior. It means that an unexplained rise in IOP on a medication you have previously responded to should prompt a conversation about which formulation you are actually using.
If your drops were controlling your pressure and your pressure has risen, the drop may not have changed, but the bottle might have.
A Note on Compliance: The Larger Picture
Glaucoma requires lifelong management. That is a long time to take a drop every evening without ever seeing any evidence that it is working: no improvement in vision, no symptom relief, nothing measurable in your daily life. The only evidence is a number on a machine in a clinic you visit every few months.
This is the fundamental challenge of glaucoma compliance. And the research confirms what every glaucoma specialist observes in clinic: adherence deteriorates over time, is worst in asymptomatic patients, and is closely linked to whether patients genuinely understand why the drops matter.
The drops matter because glaucoma is a progressive optic neuropathy: a disease of the nerve, not just the pressure. The pressure is the most modifiable risk factor we have. Lower the pressure consistently and you slow, or in many cases halt, the progression. Stop lowering it, even briefly, even unintentionally, and you give the disease an opening.
Every drop counts. Every evening. For as long as your specialist prescribes them.
What to Do If You Have Missed Doses
If you have missed one or two doses, resume your drops that evening and continue as normal. Do not double-dose to compensate. One drop per eye per evening is the correct regimen regardless of what happened the night before.
If you have been off your drops for longer, a week or more, call your specialist for a pressure check. Do not wait for your next scheduled appointment. A brief gap is usually manageable, but it needs to be assessed, not ignored.
If you have run out and cannot access your usual formulation, contact your specialist’s clinic before switching to a different brand. The switch may be perfectly fine. Or not.
When to Seek a Second Opinion
If you have been prescribed prostaglandin drops and you are uncertain why. If no one has explained what your pressure target is, what your optic nerve looks like, or what the risk of stopping your drops actually means for your specific situation: you deserve a thorough conversation. Glaucoma management is not one-size-fits-all.
Patients who come to me for a second opinion often arrive having made decisions about their medication based on incomplete information. They stopped drops that were controlling their disease. Switched brands without realising the implications. They were told their pressure was fine without being told that it was fine because of the drops.
Informed patients make better decisions. If your current care has not given you the information you need to protect your own vision, ask for it. Or find a specialist who will provide it.
Clinical Reality (What’s not always obvious)
- Not everyone responds equally—some patients need additional drops, laser, or surgery despite regular use.
- Redness, darkening of eyelids/iris, or lash growth can affect comfort and adherence.
- Missing doses matters—these drops work best with consistent, long-term use.
- More medications ≠ better control; the goal is stable optic nerve over time, not just a lower number on one visit.
6. Quick Summary Table
| Aspect | What It Means for You |
|---|---|
| Role in treatment | First-line drops for most patients with glaucoma |
| How they work | Increase fluid outflow → lower eye pressure |
| Dosing | Usually once daily (often at night) |
| Effectiveness | Strong pressure reduction in most patients |
| Common side effects | Redness, irritation, eyelash growth, periocular skin darkening |
| Long-term changes | Possible gradual iris color darkening (cosmetic, not harmful) |
| When not enough | May need additional drops, laser (SLT), or surgery |
| Adherence importance | Irregular use reduces protection against progression |
| Big picture | Helps slow damage—but needs monitoring, not blind continuation |
Frequently Asked Questions
What are prostaglandin analogues and how do they lower eye pressure?
Prostaglandin analogues are the most commonly prescribed first-line eye drops for glaucoma. They include latanoprost, bimatoprost, travoprost, and tafluprost. They work by increasing the drainage of fluid from the eye through the uveoscleral pathway, reducing intraocular pressure by 25 to 35 percent in most patients. These drops are used once daily, typically at night.
What happens if I stop my glaucoma eye drops suddenly?
When you stop prostaglandin drops, the pressure-lowering effect wears off and your intraocular pressure rises again, often higher than your original baseline. This is called a rebound IOP spike. Because glaucoma damages the optic nerve silently, this pressure rise causes harm before you feel anything. Even a brief gap in treatment can accelerate nerve fibre loss that cannot be reversed.
Is it safe to stop glaucoma drops if my eye pressure is normal?
No. Your pressure is normal because the drops are working. Stopping them removes the treatment, not the disease. Glaucoma is a chronic condition that requires lifelong pressure control. Normal pressure on medication means the medication is doing its job, not that you no longer need it.
Can I switch between generic and branded prostaglandin drops?
Not without consulting your glaucoma specialist. Research has shown significant variation in drug concentration, osmolality, and drop volume between different generic prostaglandin formulations available in India. If your chemist substitutes your usual brand, inform your doctor and have your pressure checked. An unexplained rise in IOP while on medication may be related to a formulation change.
What are the common side effects of prostaglandin eye drops?
Most patients tolerate prostaglandin drops well. Known side effects include mild redness and irritation (usually temporary), gradual darkening of the iris in patients with mixed-colour eyes, eyelash lengthening and thickening, and periorbital changes such as deepening of the upper eyelid crease with long-term use. Rare side effects include cystoid macular oedema, particularly in patients with a history of cataract surgery or uveitis. None of these are reasons to stop drops without first speaking to your specialist.
What should I do if I miss a dose of my glaucoma drops?
Resume your drops that evening and continue as normal. Do not use two drops to make up for the missed dose. The correct dose is one drop per eye per evening regardless. If you have missed drops for a week or more, contact your specialist for a pressure check rather than waiting for your next scheduled appointment.
Do I need to stop my glaucoma drops before eye surgery?
Only if your surgeon specifically instructs you to. There are situations, certain glaucoma and cataract procedures, where prostaglandin drops are paused before surgery. This decision must come from your treating doctor, with a clear plan for monitoring your pressure during any gap. If no one has told you to stop your drops, keep using them.
Why do my eyes look different after years of using glaucoma drops?
Long-term use of prostaglandin analogues can cause periorbital changes, including deepening of the upper eyelid sulcus, mild drooping of the eyelid, and loss of orbital fat. These changes are more noticeable with bimatoprost than with latanoprost or travoprost. They are not medically harmful but are worth discussing with your specialist if you notice them. Switching to a preservative-free formulation or a different molecule may reduce these effects.
Are prostaglandin drops safe for long-term use?
Yes, for the vast majority of patients. Prostaglandin analogues have a well-established long-term safety profile and are the global standard of care for first-line glaucoma treatment. The risks of stopping them, uncontrolled IOP and progressive optic nerve damage, are far greater than the risks of continuing them under specialist supervision.
When should I seek a second opinion about my glaucoma treatment?
Seek a second opinion if you do not understand why a particular drop has been prescribed, what your target pressure is, or what the risk of stopping your medication actually means for your specific optic nerve and disease stage. Patients who arrive for a second opinion often discover they have been making decisions, including stopping drops, based on incomplete information. Informed patients protect their own vision better. A thorough explanation of your diagnosis and treatment plan is not optional; it is part of good glaucoma care.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine,. This article was edited in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma