
How to Tell Myasthenia Gravis From Nerve Palsy (and Why It Matters) Fluctuating double vision often points to specific neurological…
Tag: best eye doctor in gurgaon
OCT and Visual Field
Understanding Glaucoma Investigations: OCT and Visual Field
OCT shows the structure of the optic nerve. Visual field tests show how vision is functioning. Patients struggle to understand why their doctor has reached a certain diagnosis, or treatment strategy. Many patients receive OCT and visual field reports full of colours and numbers. Both require careful interpretation, and an equally careful explanation. the truth is, your doctor is looking for a structure-function relationship, correlating it to your eye pressures, and the lifetime risk to your vision, and quality of life.
Glaucoma diagnosis is rarely based on one scan. Also glaucoma often has no symptoms. It requires understanding patterns over time: how the optic nerve looks, how visual fields change, how eye pressure behaves, and how your individual risk factors fit together.
OCT shows the structure of the optic nerve. Visual field tests show how vision is functioning.
Neither test alone can diagnose glaucoma. This is why reports sometimes seem confusing. A red area on OCT may be normal for a highly myopic eye. An abnormal visual field may simply reflect fatigue or cataract. On the other hand, subtle early glaucoma can be missed if reports are not compared carefully across months and years.
In glaucoma care, numbers do not treat disease. Understanding does.
My approach focuses on calm, structured interpretation of OCT and visual field reports so patients can make informed decisions about long-term eye health. Because glaucoma is usually invisible early, our goal is not only to see clearly today, but to protect vision safely ten years from now.
If your reports are confusing, conflicting, or leading to rushed treatment decisions, a structured glaucoma second opinion can help bring clarity.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Understanding OCT
OCT measures thickness of nerve fibres. Red areas may indicate thinning.
But interpretation depends on:
• age
• myopia
• optic nerve size
• machine variability
• baseline comparison
One abnormal OCT does not prove glaucoma. But ignoring subtle changes can be dangerous.
Understanding Visual Fields
Visual field tests measure functional vision.
But results vary with:
• patient attention
• fatigue
• learning effect
• cataract
• dry eye
One abnormal field may not mean disease. Repeated patterns matter more when evaluating progression.
Why OCT and Visual Field Reports Must Be Interpreted Together
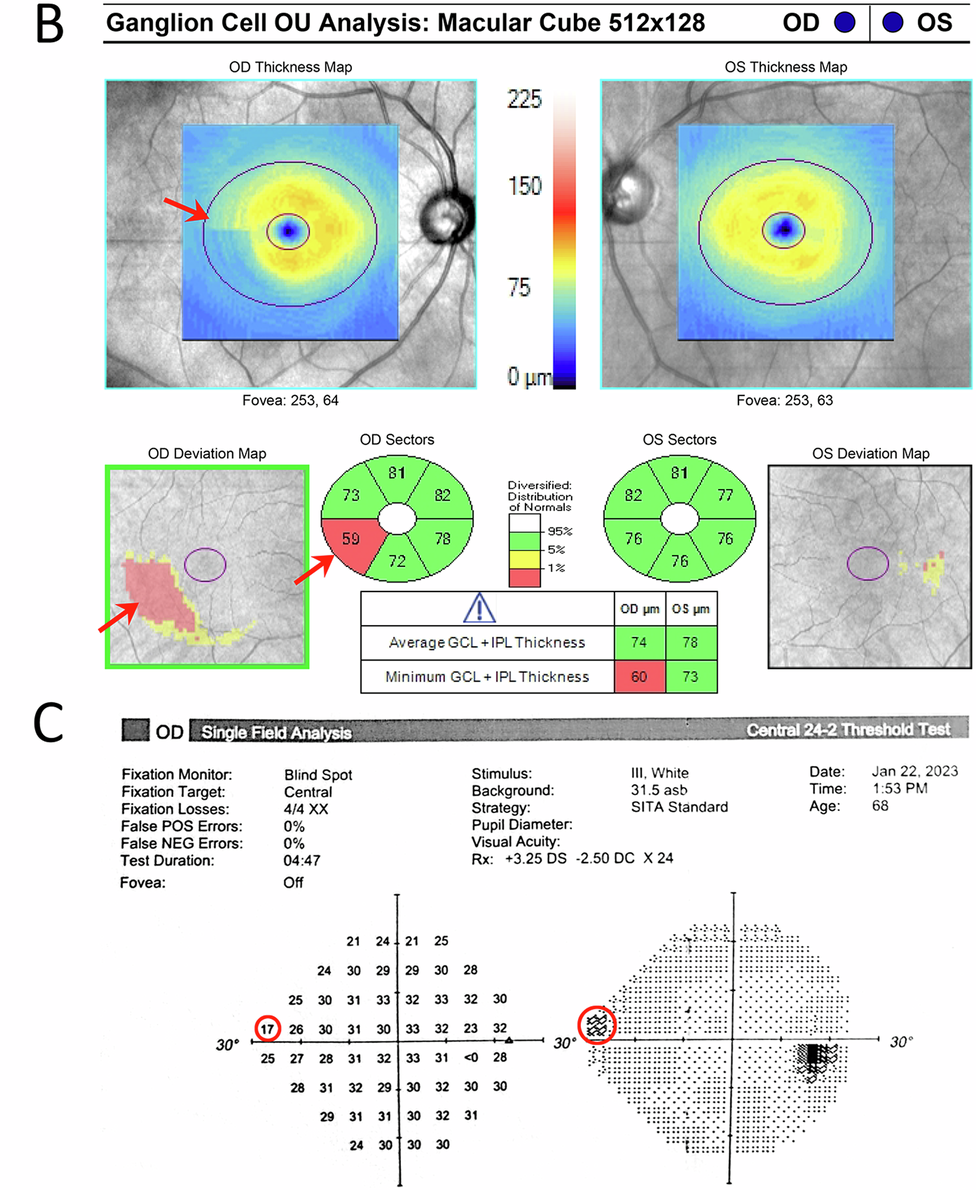
Glaucoma diagnosis needs both structure and function. OCT shows nerve structure. Visual field shows vision function. When both OCT and Visual Field show similar changes over time, diagnosis is stronger, and rooted in deeper evidence.
The Importance of Serial Comparison
The most important glaucoma test is comparison.
We compare:
• OCT over years
• visual fields over years
• optic nerve photos
Progression becomes visible only in hindsight. That is why follow-up matters.
Common Misinterpretations
• Red OCT areas in high myopia
• Field defects from cataract
• Machine artefacts
• Ignoring early thinning
You should not panic, or be falsely reassured. What you should ask for is a detailed explanation.
When to Seek Specialist Interpretation
• Conflicting reports
• Advice for surgery
• Multiple drops
• Normal pressure but abnormal OCT
• Strong family history
A structured interpretation can clarify risk.
My Approach
Reports are reviewed systematically with attention to long-term risk.
Patients receive:
• clear explanation
• risk assessment
• management options, including follow up schedule
• missing data list
Because glaucoma care is about continuity, and steady compliance with treatment.
⭐ FAQs – OCT and Visual Field Interpretation
1. My OCT report shows red areas. Does this mean I have glaucoma?
Not always. OCT compares your nerve thickness with an average database.
Red areas can appear in:
• high myopia
• large optic nerves
• normal anatomical variation
• machine artefacts
OCT is only one part of glaucoma diagnosis. It must be interpreted with visual fields, optic nerve exam, and follow-up over time.
2. My visual field test was abnormal once. Should I worry?
A single abnormal visual field does not confirm glaucoma. Visual fields depend on attention, fatigue, dry eye, cataract, and learning effect. Doctors usually repeat the test to confirm a pattern. Consistency over time matters more than one report.
3. Can OCT be normal but glaucoma still present?
Yes. No one test is infallible when it comes to glaucoma diagnosis.
Very early glaucoma can be missed on OCT, especially in normal-tension glaucoma or small optic nerves. This is why clinical examination and follow-up are important. Glaucoma diagnosis is a pattern seen over time, not one scan.
4. Can visual fields be normal if glaucoma is already present?
Yes. Structural nerve damage often occurs before functional loss. Patients may have normal visual fields but abnormal OCT or optic nerve appearance. Early detection focuses on protecting long-term vision before symptoms appear.
5. How often should OCT and visual field tests be repeated?
It depends on your risk of glaucoma progression or vision loss.
• Low risk: once a year
• Glaucoma suspect: every 6–12 months
• Established glaucoma: every 3–6 months
Your doctor decides based on progression risk. Regular comparison (and therefore, regular follow up) is the most important part of glaucoma care.
6. Why do my OCT numbers change between tests?
Small changes happen because of:
• machine differences
• scan alignment and test retest variability
• eye dryness
• cataract
• natural variation
Doctors thus look for consistent trends, not small fluctuations.
7. Can cataract affect visual field results?
Yes.
Cataract can cause diffuse depression on visual field testing. This may look like glaucoma but improves after cataract surgery. This is why reports must be interpreted carefully.
8. My eye pressure is normal. Why do I need OCT and Visual Field?
Many patients have normal-tension glaucoma. Pressure alone cannot rule out disease. OCT and visual field testing help detect subtle nerve damage. Glaucoma diagnosis needs multiple data points, eye pressure is only one of them.
9. Can glaucoma tests (OCT and Visual field) be wrong?
Tests are not “wrong,” but they can be misleading if taken in isolation. Machines measure data. Doctors interpret patterns. Also, visual fields can have fixation losses (you looked away from the fixation light), as well as false positives and false negatives. High rates of any of these can make your visual fields unreliable.
A structured review reduces unnecessary treatment and dangerous delay.
10. When should I seek a glaucoma second opinion?
Consider a second opinion if:
• You are advised surgery suddenly
• Reports are confusing
• Multiple drops are started without explanation
• OCT and visual field results disagree
• Strong family history exists
Clarity helps you make calm, informed decisions.
11. What is the most important glaucoma test?
The most important test is comparison over time. Glaucoma progression becomes visible only when reports are compared across months and years. Continuity of care is essential, and one all clear diagnosis does not mean you don’t need a follow up visit.
Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides trusted second opinions for patients seeking clarity before major treatment decisions. Both, in person, and online.
12. Can glaucoma be cured if detected early?
Glaucoma cannot be reversed. But early detection and regular care can preserve useful vision for life. The goal is not perfect tests today, but safe vision ten years from now, and always.
Closing Thought
Numbers do not treat glaucoma.
Understanding does.
Protecting vision requires careful interpretation over time.
If you would like your OCT or visual field reports reviewed in a structured glaucoma second opinion:
📞 +91 88826 38735
🌐 drshibalbhartiya.com
Second Opinion Form for teleconsults
Related Reading
- Why Do I Need a Visual Field Test?
- Understanding Your OCT Report in Glaucoma
- Visual Field and OCT: Structure & Function Correlation
- Glaucoma Diagnosis in Gurgaon
- Glaucoma Progression: What It Means and How to Slow It
- Get a Glaucoma Second Opinion in Gurgaon
- Get an Online Glaucoma Consult
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
For people unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma

Is Glaucoma Hereditary?
Glaucoma is hereditary. This means that if someone in your family, especially a first degree relative, has glaucoma, your risk for developing glaucoma is definitely higher than the general population.
Types of Glaucoma: Open Angle, Closed Angle, Normal Tension, and More
Types of Glaucoma: Open Angle, Closed Angle, Normal Tension, and More, explained by Dr Shibal Bhartiya, glaucoma specialist in Gurgaon.
Glaucoma is not a single disease. It is a family of conditions, each with different causes, risk factors, and treatment approaches. What they share is a common outcome: damage to the optic nerve, leading to progressive and irreversible vision loss if untreated.
Understanding which type of glaucoma you have helps you ask better questions and follow your treatment plan with more confidence. This page explains the main types, from the most common to the less well known, written for patients rather than clinicians.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Not all glaucomas behave the same way, and the treatment that is right for open-angle glaucoma may be wrong for angle-closure or normal tension glaucoma. Getting the diagnosis right, and the type right, is where good glaucoma care begins.
If you are uncertain about your diagnosis, a structured second opinion can bring clarity.
THE TWO MAIN TYPES OF GLAUCOMA
Q1. What is the difference between open-angle and closed-angle glaucoma?
Most glaucomas fall into one of two broad categories, determined by the anatomy of the drainage angle of the eye.
Open-angle glaucoma is by far the more common type of glaucoma. The drainage angle is open and appears normal, but fluid drains too slowly, causing pressure to build gradually over months and years. It has no symptoms in the early stages. Patients typically lose peripheral vision first, and the brain compensates so well that many people do not notice the loss until the disease is advanced. This is why regular screening is essential, particularly for those with risk factors.
Closed-angle glaucoma occurs when the drainage angle is narrow or blocked, preventing fluid from draining. It can occur suddenly (acute angle closure) or gradually (chronic angle closure). The acute form is a medical emergency with symptoms including severe eye pain, redness, blurred vision, and nausea. The chronic form is subtler and may mimic open-angle glaucoma.
Note: The distinction between the two types of glaucoma (open and closed angle) is made using a test called gonioscopy. This single test shapes all subsequent treatment decisions.
CLOSED-ANGLE GLAUCOMA
Q2. I have been diagnosed with angle-closure glaucoma. What does that mean for me?
In angle-closure glaucoma, the iris (the coloured part of the eye) is too close to the drainage angle, narrowing or blocking it. When the angle closes, fluid cannot drain and eye pressure rises sharply.
The acute form causes a sudden, severe rise in pressure. Symptoms include a red, painful eye with blurred vision, coloured halos around lights, headache, and nausea. This is an eye emergency; seek immediate medical help if this happens.
The chronic form builds more slowly, with few symptoms other than occasional coloured halos and mild headaches. It can go undetected for years without a formal eye examination.
Treatment for angle-closure glaucoma starts with a laser procedure called laser peripheral iridotomy (LPI). This creates a small opening in the iris to provide an alternative drainage pathway. After LPI, some patients require no further treatment; others need long-term eye drops. Your doctor will monitor your pressure and angle anatomy over time.
Note: Family members of patients with angle-closure glaucoma have a higher risk of the same condition. Preventive laser iridotomy can be offered to at-risk relatives before any acute episode occurs.
NORMAL TENSION GLAUCOMA
Q3. My doctor says I have glaucoma, but my eye pressures are normal. How is that possible?
This is understandably confusing. Between 10 and 25 percent of people with glaucoma have eye pressures that fall within the normal range (below 21 mmHg). This is called normal tension glaucoma (NTG), or low tension glaucoma.
The exact cause is not fully understood. Two leading theories are that the optic nerve is unusually sensitive to pressure and sustains damage even at pressures that would be harmless in most people, or that the blood supply to the optic nerve is compromised, making it vulnerable to damage independent of pressure. Of all the types of glaucoma, this is perhaps the most confusing for patients.
Conditions associated with normal tension glaucoma include:
- Japanese ancestry (NTG is significantly more common in East Asian populations)
- A family history of normal tension glaucoma
- Migraines and vasospastic disorders such as Raynaud’s disease
- Sleep apnoea
- Alzheimer’s disease
Treatment still focuses on lowering eye pressure, like all other types of glaucoma. Even when eye pressure is within the normal range to start with, clinical trials have shown this slows progression. Eye drops, laser, or surgery may be used depending on the rate of progression and individual risk factors.
Note: Normal tension glaucoma often progresses more slowly than high-pressure glaucoma, but regular monitoring is still essential. Missing follow-up appointments is the most common reason for avoidable vision loss.
OCULAR HYPERTENSION
Q4. My eye pressures are high but my doctor says I do not have glaucoma. What is ocular hypertension?
If your eye pressure is above the normal range but your optic nerve and visual field show no signs of damage, you have ocular hypertension (OHT). It is not glaucoma, but it is a significant risk factor for developing glaucoma.
Not everyone with high eye pressure will develop glaucoma. Your individual risk depends on your age, ethnicity, family history, and corneal thickness (thicker corneas can give falsely high pressure readings).
Your doctor will weigh your risk profile before deciding whether to treat. Options include eye drops or selective laser trabeculoplasty (SLT). In lower-risk patients, careful monitoring without treatment is often appropriate, since all glaucoma medications carry some side effect burden.
Whether or not you receive treatment, regular eye checks are essential. The goal is to detect any optic nerve or visual field changes before significant vision is lost. Knowing your risk early is one of the best things you can do for your vision.
GLAUCOMA SUSPECT
Q5. My doctor says I am a glaucoma suspect. My tests were normal. Why do I still need annual monitoring?
A glaucoma suspect is someone whose optic nerve appearance raises concern, even when eye pressure and visual field tests are currently normal.
The most common reason is a larger than average cup-to-disc ratio (the proportion of the optic nerve head occupied by the central cup). A ratio above 0.5, or a difference of 20 percent or more between the two eyes, warrants closer monitoring. Other reasons include borderline eye pressures or a strong family history of glaucoma.
This does not mean you have glaucoma. It means your doctor wants a baseline record to compare against over time. If the optic nerve or visual field changes, that change can be detected early and treatment started before significant vision is lost.
Most glaucoma suspects are asked to return for annual or biannual testing. Once several years of stable results have been recorded, the interval between visits may be extended.
Note: The value of being labelled a glaucoma suspect is that it keeps you in the system. Early detection is the single most powerful tool for preventing glaucoma blindness.
SECONDARY GLAUCOMA
Q6. What is secondary glaucoma, and what causes it?
Secondary glaucoma is glaucoma caused by another identifiable condition or event, rather than arising on its own. It is managed in the same way as primary glaucoma (eye drops, laser, or surgery), but the underlying cause must also be addressed.
The most common secondary types of glaucoma include:
- Pseudoexfoliation glaucoma: A protein-like material deposits on the lens and drainage structures of the eye, blocking outflow. This is one of the most common secondary glaucomas in India and tends to cause higher pressures and faster progression than primary open-angle glaucoma. It requires close monitoring and often more aggressive treatment.
- Pigmentary glaucoma: Pigment granules shed from the back of the iris clog the drainage angle. It typically affects younger, myopic (short-sighted) patients and is often missed because these patients are not in the standard high-risk age group for glaucoma screening.
- Steroid-induced glaucoma: Long-term use of steroid eye drops, nasal sprays, skin creams, or oral steroids can raise eye pressure in susceptible individuals. If you are on any form of steroid medication for any condition, ask your doctor whether your eye pressure has been checked.
- Traumatic glaucoma: An injury to the eye can damage the drainage angle and cause pressure to rise, sometimes years after the original injury. Any history of significant eye trauma should be disclosed to your eye doctor.
- Neovascular glaucoma: New, abnormal blood vessels grow over the drainage angle, blocking outflow. It is most commonly associated with poorly controlled diabetes and retinal vein occlusion. It is one of the more difficult types to manage and often requires surgery.
Note: If you have a systemic condition such as diabetes, or are on long-term steroid medication, make sure your eye doctor is aware. These are glaucoma risk factors that are often overlooked.
CONGENITAL AND CHILDHOOD GLAUCOMA
Q7. My child has been diagnosed with glaucoma. How is that possible, and what should I expect?
Glaucoma can affect any age group, though it is most common in adults over 40. In children, the most common cause is a structural defect in the drainage angle that is present from birth; this is called congenital glaucoma or primary infantile glaucoma.
Signs that parents typically notice first include:
- Cloudy or hazy eyes
- Unusual sensitivity to light; the child may turn away from bright light or bury their face
- Excessive tearing
- Eyes that appear larger than normal (because raised pressure causes the infant eye to expand)
Eye drops may be started initially to control pressure, but surgery is almost always required for congenital glaucoma. Early surgical intervention gives the best chance of preserving good vision throughout the child’s life.
Some children also have a co-existing cataract or other eye abnormality that needs to be managed alongside the glaucoma. Glasses, patching therapy for amblyopia (lazy eye), and follow-up surgeries may all be part of the long-term plan.
Children with glaucoma can lead fully independent lives. Even where some vision has been lost, tailored rehabilitation and visual aids allow children to participate in all age-appropriate activities. As a parent, remaining engaged with the care team and encouraging the child’s independence are the most important things you can do.
Note: Congenital glaucoma is rare. If your child has been diagnosed, seek care from a specialist with specific paediatric glaucoma experience. Early and consistent follow-up is critical.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. This article was edited in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Available on Pubmed and Google Scholar
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
Patient reviews Google Business Profile
Glaucoma FAQs: Expert Answers from a Glaucoma Specialist in Gurgaon
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care.
These answers are drawn from real questions patients bring to the clinic: at first diagnosis, during follow-up, and when seeking a structured glaucoma second opinion in Gurgaon. If you do not find what you are looking for here, reach out directly.
What is glaucoma? Can it be prevented?
Glaucoma is a group of eye diseases that damage the optic nerve, causing progressive and irreversible vision loss. It is the second most common cause of blindness worldwide. Most people have no symptoms until significant damage has already occurred.
Glaucoma cannot be prevented. However, early detection and consistent treatment can slow progression and protect functional vision for life. The key is finding it before the damage is done. This is why regular screening matters, especially if you carry a family history of glaucoma.
Glaucoma tests are painless. A standard screening includes a vision check and eye pressure measurement. Depending on your risk profile, your doctor may also recommend a visual field test, an OCT scan to measure nerve fibre thickness, and a gonioscopy to examine the drainage angle of the eye. Learn more about glaucoma diagnosis in Gurgaon.
What puts me at risk for glaucoma?
Anyone above 40 should have an annual eye check. The following risk factors increase urgency significantly:
- Family history of glaucoma — the single strongest risk factor
- History of eye injury or trauma
- Long-term use of steroid medications, including eye drops, inhalers, or oral steroids
- Diabetes or thyroid disease
- History of migraines or vasospastic disorders such as Raynaud’s disease
- Sleep apnea
- Alzheimer’s disease
- High myopia (shortsightedness) or high hypermetropia (longsightedness)
- Symptoms such as frequent prescription changes, coloured haloes around lights, headaches with nausea, or sudden blurring of vision
Vision lost to glaucoma cannot be recovered. Once nerve fibres are gone, they do not grow back. Regular eye exams are not optional if you carry these risk factors, they are what stand between you and preventable blindness. Understand glaucoma risk in depth here.
What happens during a glaucoma check-up?
Bring all previous eye records, your current glasses, any eye drops you are using, and your full medical file: not just eye records. Conditions such as diabetes, blood pressure, and thyroid disease all have relevance to glaucoma management.
Before you see the doctor, an optometrist will check your vision and eye pressure. Your doctor will then examine your optic nerve and retina. Additional tests may include a visual field test, an OCT scan, pachymetry (corneal thickness), a water drinking test, and a dilated eye exam.
After the tests, your doctor will explain findings clearly and outline a plan. Do not drive yourself to the appointment: your eyes may be dilated, which blurs vision for approximately three hours. Bring sunglasses.
I have glaucoma. Will I go blind?
In most cases, no- provided care is consistent. With proper medical care, glaucoma blindness is avoidable. Patients who use their eye drops as prescribed, attend follow-up appointments, and respond to treatment adjustments generally retain their vision for life.
The variables that matter most are: how early the disease was detected, how well eye pressure is controlled, and how reliably treatment is continued. Glaucoma is not a condition where you treat it and forget it. It requires steady, long-term management.
If glaucoma has advanced significantly, surgery may be recommended to slow further progression. In cases with severe visual field constriction, low vision aids can support daily mobility and independence.
The most important thing you can do today is ask your doctor honest questions about your disease stage and what your realistic prognosis looks like with good adherence. Lifestyle changes that support glaucoma management are discussed here.
How often should I see my doctor after a glaucoma diagnosis?
Frequency depends on disease severity, eye pressure control, and how stable your condition is. Here is a general framework:
- Glaucoma suspect: Annual review with full testing, more often if your doctor recommends it
- Early glaucoma, well-controlled: Every 6 to 12 months
- Moderate or advanced glaucoma, or poorly controlled pressure: Every 3 to 6 months
- After surgery: Intensive early follow-up, then gradual spacing as the eye stabilises
Even after surgery, eye drops may still be needed. Even if pressure is well-controlled, regular visits remain essential. Glaucoma can change silently. Gaps in follow-up are where damage accumulates.
If you are unsure whether your current follow-up schedule is appropriate, a structured glaucoma second opinion can provide clarity on both disease status and the right monitoring plan. Read more about glaucoma treatment planning here.
How can I support a family member or partner who has glaucoma?
A glaucoma diagnosis can be frightening. The word carries the weight of possible blindness, even when the actual prognosis with treatment is good. Your most important role early on is reassurance: with consistent care, blindness is not the inevitable outcome.
Practically, you can help by:
- Reminding them to use their eye drops at the same time each day
- Driving them to clinic appointments, particularly when eyes are dilated
- Helping them track and attend follow-up visits
- Learning enough about the condition to ask informed questions during consultations
- Help them manage anxiety and depression through support, and medical help when required
If your family member has significant visual impairment, discuss visual rehabilitation options and low vision aids with their doctor. Support groups and rehabilitation services exist specifically for this. You do not have to navigate it alone. Read more about glaucoma and quality of life here.
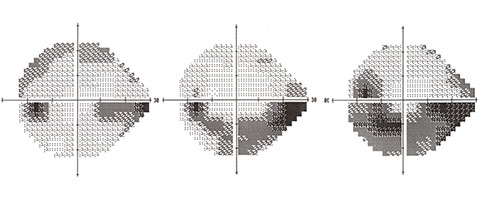
What does vision loss from glaucoma actually feel like?
This is one of the most important, and most misunderstood, aspects of glaucoma. Most patients feel nothing. Even significant visual field loss often goes unnoticed because the brain compensates automatically by filling in missing areas. This is why patients sometimes underestimate their own disease severity.
The Glaucoma SIM App, developed in partnership with MSD Pharmaceuticals, the International Glaucoma Association, and Moorfields Eye Hospital, allows you to simulate what progressive glaucoma field loss looks like over time. It is available on the Apple App Store (search: Glaucoma SIM). Verify availability for your region before downloading.
Understanding what is happening to your vision, even when you cannot feel it, is one of the strongest motivators for staying consistent with treatment.
How do I choose a glaucoma doctor? When should I seek a second opinion?
A good glaucoma specialist listens carefully, explains your diagnosis in plain language, and makes treatment decisions transparently. Credentials matter: look for fellowship training in glaucoma, peer-reviewed publications, and clinical experience with complex cases including surgery.
A second opinion is not a sign of distrust. It is a standard part of managing a serious, lifelong condition. Seek one proactively if:
- You have been recently diagnosed and want to confirm the findings
- Your disease appears to be progressing despite treatment
- Surgery has been recommended and you want to understand all your options
- You are uncertain about your current treatment plan or follow-up schedule
- You have seen multiple doctors and received different advice
Dr Shibal Bhartiya offers structured glaucoma second opinions in Gurgaon, as well as online consultations for patients elsewhere in India. She works in partnership with your local doctor to guide care over time- you do not need to change your primary treating physician. Submit a second opinion request here.
What are reliable resources for learning more about glaucoma?
Use these trusted sources for current, evidence-based information:
- American Academy of Ophthalmology — clinical guidelines and patient education
- National Eye Institute (NEI) — US National Institutes of Health glaucoma resource
- Glaucoma Research Foundation — patient-facing information and research updates
- World Glaucoma Association — global clinical standards
- ClinicalTrials.gov — ongoing research trials
- PubMed — peer-reviewed literature, including Dr Shibal Bhartiya’s published research
- Knowledge Series on this site — articles written by Dr Bhartiya for patients and caregivers
- Dr Bhartiya talks to one of her patients in this video, and answers her questions.
Book a Glaucoma Evaluation or Second Opinion
Not sure about your diagnosis? Concerned about progression? Want clarity before agreeing to surgery? Dr Shibal Bhartiya brings over 25 years of fellowship-trained glaucoma expertise, Mayo Clinic research collaboration, and 90+ peer-reviewed publications to every patient evaluation.
Consultations are available in person at Marengo Asia Hospitals, Sector 56, Gurgaon, and online for patients outside the city. Book an appointment here or call +91 88826 38735. You can also submit a second opinion request online.
For patients who live elsewhere, Dr Bhartiya is happy to work in partnership with your local eye doctor to guide and support your care over time.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. This article was edited in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Available on Pubmed and Google Scholar
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
Patient reviews Google Business Profile