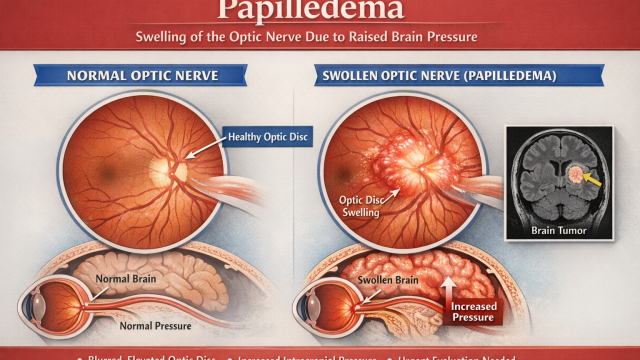
Papilledema is swelling of the optic nerve caused by increased pressure inside the brain. It can signal serious conditions like brain tumours or raised intracranial pressure and needs urgent evaluation.
Understanding this matters:
- Papilledema is not just an eye disease, it is an eye sign of brain disease
- It is a sign of increased pressure inside the skull
The eye is simply where this pressure becomes visible, says Dr Bhartiya.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
Why Papilledema Matters
Raised intracranial pressure can occur due to:
- Idiopathic intracranial hypertension (IIH)
- Brain tumours or space-occupying lesions
- Intracranial bleeding
- Cerebral venous sinus thrombosis
- Severe head injury
- Hydrocephalus
- Central nervous system infections
Papilledema may be the first detectable sign of these conditions.
Missing it can lead to:
- Permanent vision loss
- Progressive optic nerve damage
- Delayed diagnosis of serious neurological disease
Clinically speaking, the most common cause of papilledema today is: Idiopathic Intracranial Hypertension (IIH, also called BIH or pseudotumor cerebri) Across neuro-ophthalmology clinics worldwide, IIH is now the single most frequent diagnosis when papilledema is detected — especially in eye clinics.
The most common reason we see this kind of optic nerve swelling is a condition where brain pressure is a bit higher than normal, without any underlying pathology. It’s usually treatable with medication onlu, but we always do careful tests first to be safe.
Typical profile:
- Women of reproductive age
- Overweight or recent weight gain
- Chronic headaches ± transient visual symptoms
- Normal brain imaging (no mass lesion)
- Elevated CSF opening pressure on lumbar puncture
Crucially:
- Vision may be normal early
- Papilledema may be the only objective sign
- Delay risks permanent optic nerve damage
However, Very Important to Note
Although IIH is the most common, papilledema must never be assumed to be IIH upfront.
Before calling it idiopathic, you must exclude:
- Brain tumour or space-occupying lesion
- Cerebral venous sinus thrombosis
- Hydrocephalus
- Intracranial bleed or infection
That exclusion step is non-negotiable.A common misconception
“My vision is fine, so it can’t be serious.”
This is false.
In early and even moderate papilledema:
- Central vision may be normal
- Visual acuity may be 6/6
- The patient may not complain of vision loss
Vision loss often appears late, after damage has already occurred.
Symptoms of Papilledema
Some patients have no visual symptoms at all.
Others may report:
- Headache (often worse on waking)
- Transient visual blurring, especially on standing
- Brief episodes of vision blacking out
- Nausea or vomiting
- Pulsatile tinnitus (whooshing sound in the ear)
- Double vision (from sixth nerve palsy)
The absence of symptoms does not rule out papilledema.
How Papilledema is Different from Optic Neuritis
This distinction is critical and often confused.
| Feature | Papilledema | Optic Neuritis |
|---|---|---|
| Cause | Raised intracranial pressure | Inflammation of optic nerve |
| Pain | Usually painless | Often painful on eye movement |
| Vision loss | Late | Early |
| Laterality | Usually bilateral | Often unilateral |
| Urgency | Neurological emergency | Neurological evaluation needed |
Treating papilledema as optic neuritis — or vice versa — can be harmful.
How Papilledema is Diagnosed
Diagnosis begins with a careful optic nerve examination.
Key steps include:
- Detailed fundus evaluation
- Documentation of optic disc margins
- Assessment for haemorrhages or exudates
- Visual field testing (often shows enlarged blind spots)
- Optical coherence tomography (OCT) to document nerve fibre swelling
Once suspected, urgent neuro-imaging is required before further intervention.
A lumbar puncture is performed only after imaging, never before.
Why “just a headache” is not reassuring
Headache is common.
Papilledema is not.
When headache is accompanied by:
- optic nerve swelling
- transient visual symptoms
- sixth nerve palsy
- unexplained visual complaints
it requires escalation in these cases, not reassurance.
Treatment Principles
Papilledema itself is not treated directly.
Management focuses on:
- Identifying the cause of raised intracranial pressure
- Reducing pressure safely
- Preventing optic nerve damage
- Coordinated care between neurology, neurosurgery, and ophthalmology
Delays increase the risk of field defects and even permanent visual loss.
When to Seek Urgent Evaluation
Immediate assessment is required if:
- Papilledema is suspected on eye examination
- Headache is progressive or associated with visual symptoms
- There is double vision, vomiting, or altered consciousness
- Vision fluctuates or dims transiently
Waiting for symptoms to worsen is unsafe.
Key Take-Home Message
Papilledema is a neurological warning sign, not an eye diagnosis.
Good vision does not mean safety.
A normal eye test without optic nerve examination is incomplete.
The most common reason we see this kind of optic nerve swelling is a condition where brain pressure is a bit higher than normal, without any underlying pathology. It’s usually treatable with medication only, but we always do careful tests first to be safe. Early recognition protects both vision and life in case of any underlying pathology.
Read the research articles
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on eye care management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation