If your eye test says your vision is “normal” but you still struggle with reading, driving at night, or navigating daily life, you’re not imagining it. Many early eye conditions, especially glaucoma and neuro-visual issues, affect how you function in real-world settings long before they affect standard vision test results. Dr Shibal Bhartiya explains more.
Dr Shibal Bhartiya is a fellowship-trained glaucoma specialist, and neuro-ophthalmologist; and Mayo Clinic Research Collaborator with over 25 years of experience. Her approach focuses on identifying risk before damage is irreversible, simplifying treatment decisions, and protecting vision long-term. Emphasis on early detection, risk assessment, and continuity of care. She is rated 5 stars across 1,500+ patient reviews on Google.
You’re Not Alone, and You’re Not Overthinking It
A very common experience patients describe is this:
- “My reports are normal.”
- “The doctor says I can see well.”
- “But something still feels off.”
You may notice:
- Difficulty reading for long periods
- Trouble driving at night
- Feeling slower or less confident navigating spaces
- Increased eye strain or fatigue
- Subtle “disconnect” between what you see and how you function
These symptoms are real, even if your test results look fine.
What Standard Eye Tests Actually Measure
Most clinic-based vision testing focuses on:
- Visual acuity (reading letters on a chart)
- Basic refraction (glasses power)
- Structural imaging (like OCT scans)
- Snapshot visual fields
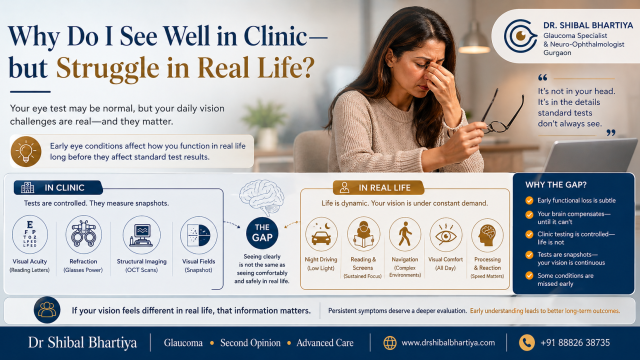
These are important, but they are not designed to fully capture how you use vision in daily life.
The Gap: “Seeing Clearly” vs “Seeing Comfortably and Safely”
There’s a critical difference:
- Seeing clearly = You can read letters on a chart
- Seeing functionally = You can navigate, read, react, and sustain vision in real life
Many early eye conditions affect the second long before the first.
Why Real-Life Vision Can Feel Worse Than Clinic Vision
1. Early Functional Loss Is Subtle
Conditions like glaucoma often begin with:
- Reduced contrast sensitivity
- Difficulty in dim lighting
- Slower visual processing
These do not show up clearly in routine tests early on.
2. Your Brain Compensates; Until It Can’t
The visual system is remarkably adaptive.
- You may unconsciously adjust posture, speed, or attention
- The brain fills in gaps in vision
- This creates a false sense of “normalcy” on testing
But in real-world conditions, complex, dynamic, unpredictable, this compensation breaks down.
3. Clinic Testing Is Controlled, Life Is Not
In clinic:
- Lighting is optimal
- Targets are high contrast
- There are no distractions
In real life:
- Lighting varies
- Movement is constant
- Visual demands are complex
Your symptoms often show up only outside the clinic environment.
4. Tests Are Snapshots, Your Vision Is Continuous
Most tests capture a moment.
But your visual experience is:
- Long-duration
- Fatigue-dependent
- Context-sensitive
That’s why you may “pass” a test, but still struggle over time.
5. Some Conditions Are Missed Early
This pattern is especially common in:
- Early glaucoma
- Neuro-ophthalmic conditions
- Visual processing issues
- Early optic nerve dysfunction
In these cases, structure or acuity may look normal initially, while function is already affected.
6. Early Presbyopia (Even Before You’re “Officially” Presbyopic)
You don’t have to be “40+ with reading glasses” for presbyopia to start affecting you.
In its early stages, presbyopia often presents as:
- Needing more effort to read
- Holding things slightly farther away
- Feeling more comfortable in brighter light
- Intermittent blur that comes and goes
What’s important is this:
standard clinic testing is usually done in well-lit conditions, with short-duration tasks.
In real life:
- Lighting varies (especially indoors or at night)
- Reading is sustained (phones, laptops, paperwork)
- Visual demand is continuous
Brighter ambient light helps because it:
- Improves depth of focus
- Reduces strain on the focusing system
- Temporarily compensates for early loss of accommodation
So you may “see fine” in clinic, but struggle in everyday, dimmer environments.
7. Latent Refractive Errors (Hidden, Compensated Power Issues)
Not all refractive errors show up clearly on routine testing.
Some remain latent, meaning:
- Your eyes compensate for them during short tests
- They become apparent only with fatigue or prolonged use
This is especially relevant for:
- Low hyperopia (hidden farsightedness)
- Small amounts of astigmatism
- Early accommodative fatigue
In clinic:
- You’re alert
- Testing is brief
- Your focusing system compensates effectively
In real life:
- Visual demand is sustained
- Fatigue builds up
- Compensation breaks down
This leads to:
- Fluctuating clarity
- Eye strain
- Headaches
- A sense that “vision is not stable”
Again, the reports may look “normal”, but your experience is telling a different story.
When This Matters Most
You should take this seriously if you notice:
- Increasing effort in reading or screen use
- Difficulty with night driving
- Subtle navigation hesitation
- Frequent prescription changes
- A feeling that “something isn’t right” despite reassurance
These are often early signals, not late disease.
What Should You Do Next?
Instead of repeating the same basic tests, the goal is to change the way your vision is evaluated.
This may include:
- Functional vision assessment
- Careful longitudinal comparison (not single reports)
- Risk-based evaluation (family history, optic nerve structure)
- Contextual interpretation, not isolated numbers
The Key Insight
If your vision feels different in real life, that information matters.
Not all vision problems are visible on routine tests, especially early.
The question is not:
“Are your reports normal?”
The question is:
“Does your vision match your life?”
When to Seek a Second Opinion
Consider a deeper evaluation if:
- Your symptoms persist despite “normal” reports
- You’ve been reassured repeatedly without explanation
- Your daily function is changing
- You want a long-term risk perspective, not just a snapshot
Evidence & Clinical Context
Emerging research reinforces that glaucoma, and visual dysfunction more broadly, is not just a disease of measurable deficits, but of lived experience. A recent study that Dr Shibal Bhartiya co-authored with her colleagues, using the GQL-15 framework, highlights how patients’ real-world visual function and quality of life can differ significantly from what standard clinical measures capture, particularly in domains like mobility, lighting adaptation, and sustained visual tasks. This aligns with what many patients report: normal test results do not always reflect how vision performs in everyday life. Interpreting vision through both objective testing and patient-reported experience is therefore critical to identifying early dysfunction and preventing long-term loss.
Remember
If your tests say everything is fine, but your experience says otherwise-that gap is worth understanding early, not dismissing.
Known for her structured approach to glaucoma risk assessment and progression analysis, Dr Shibal Bhartiya provides trusted second opinions for patients seeking clarity before major treatment decisions. Both, in person, and online.
FAQs
1. Can I have an eye problem even if my vision test is normal?
Yes. Many early eye conditions affect function (like contrast or processing) before affecting visual acuity.
2. Why do I struggle more at night if my eyes are “normal”?
Low-light conditions expose early visual system weaknesses, especially in glaucoma and optic nerve conditions. Also in early stages of presbyopia, and with latent refractive errors, you may require more ambient light for comfortable vision.
3. Are routine eye tests enough to detect all problems?
No. They are essential, but they may miss early or subtle functional changes.
4. What is the difference between vision clarity and visual function?
Clarity is your ability to read letters; function is how well you use vision in real-world situations.
5. Should I ignore symptoms if my doctor says everything is fine?
No. Persistent symptoms deserve deeper evaluation, even if initial tests are normal.
6. Can glaucoma present like this?
Yes. Early glaucoma often affects real-world vision before it shows clearly on standard tests.
7. What kind of doctor should I consult?
A glaucoma specialist or neuro-ophthalmologist who focuses on functional and longitudinal assessment.
About the Author
This article was written by Dr Shibal Bhartiya, fellowship-trained glaucoma specialist and Mayo Clinic Research Collaborator, Clinical Director at Marengo Asia Hospitals, Gurugram, known for ethical, patient-centred glaucoma care and independent glaucoma second opinions. She is also the Program Director for Community Outreach & Wellness; and for the Marengo Asia International Institute of Neuro and Spine. This article was updated in April 2026.
She has published peer-reviewed research on glaucoma management, examining how treatment decisions should balance medical evidence, patient preferences, and long-term vision outcomes.
As Editor-in-Chief of Clinical and Experimental Vision and Eye Research and Executive Editor of the Journal of Current Glaucoma Practice (Pubmed Indexed, official journal of the International Society of Glaucoma Surgery), Dr Shibal Bhartiya brings editorial and research depth to every clinical decision. Her 200+ publications, including 90+ PubMed-indexed publications and 28 edited textbooks span glaucoma biology, surgical outcomes, health equity, and emerging diagnostics.
Access her work on Pubmed, Google Scholar, ResearchGate and ORCID.
Dr Shibal Bhartiya
Glaucoma • Second Opinion • Advanced Care
www.drshibalbhartiya.com
+91 88826 38735
1500+ Five Star Patient Reviews Google Business Profile
Upload your reports for a structured review.
If you are unable to come to Dr Bhartiya’s clinic: Read more about teleconsultation for glaucoma